Vous aimerez peut-être aussi
- Unbelievably Good Gluten Free RecipesDocument14 pagesUnbelievably Good Gluten Free Recipeslaura4076Pas encore d'évaluation
- The Gluten-Free Cookbook SamplerDocument20 pagesThe Gluten-Free Cookbook SamplerSterling Publishing100% (2)
- Sinus Diet: A Beginner's Step-by-Step Guide to Managing Sinusitis and Other Sinus Symptoms Through Nutrition: With Curated Recipes and a Meal PlanD'EverandSinus Diet: A Beginner's Step-by-Step Guide to Managing Sinusitis and Other Sinus Symptoms Through Nutrition: With Curated Recipes and a Meal PlanPas encore d'évaluation
- Gluten-Free Made Easy As 1,2,3 LittleFairyRGDocument110 pagesGluten-Free Made Easy As 1,2,3 LittleFairyRGBobanBisercic100% (3)
- Group 1 Loaded Sweet Potato Rounds Prep Time: 15 Mins Cookingtime: 20 Mins Yield: 8 IngredientsDocument9 pagesGroup 1 Loaded Sweet Potato Rounds Prep Time: 15 Mins Cookingtime: 20 Mins Yield: 8 IngredientsJohn OpeñaPas encore d'évaluation
- Gluten Free HandbookDocument15 pagesGluten Free Handbookjasonh89Pas encore d'évaluation
- Gluten Intolerance Guide - Celiac DiseaseDocument3 pagesGluten Intolerance Guide - Celiac Diseasehorizon_helenPas encore d'évaluation
- Gluten CookBookDocument225 pagesGluten CookBookBoki Boris100% (6)
- Wheat Gluten and Health Powerpoint PresentationDocument22 pagesWheat Gluten and Health Powerpoint PresentationCeliaPas encore d'évaluation
- Gluten-Free Recipes For The Conscious Cook Vegetarian - Leslie CerierDocument292 pagesGluten-Free Recipes For The Conscious Cook Vegetarian - Leslie Cerierdoppler_Pas encore d'évaluation
- Meatless Monday Healthy RecipesDocument44 pagesMeatless Monday Healthy RecipesStefan Covaci100% (1)
- Natural Anti Viral Self Defense StevenWmFowkesDocument251 pagesNatural Anti Viral Self Defense StevenWmFowkesChristopher Phillips100% (1)
- Anti Candida Diet Anita SupeDocument19 pagesAnti Candida Diet Anita SupechamomilaPas encore d'évaluation
- Paleo SmoothiesDocument228 pagesPaleo Smoothieseddie0384100% (3)
- Healthy Desserts Ebook 2019 PDFDocument7 pagesHealthy Desserts Ebook 2019 PDFaPas encore d'évaluation
- Recipes From The Dairy-Free and Gluten-Free Kitchen by Denise JardineDocument13 pagesRecipes From The Dairy-Free and Gluten-Free Kitchen by Denise JardineThe Recipe Club0% (1)
- Complete Guide To Vegan Food Ebook PDFDocument14 pagesComplete Guide To Vegan Food Ebook PDFAlessia ȚernaPas encore d'évaluation
- SurefireWays PDFDocument147 pagesSurefireWays PDFedyrio100% (4)
- 2018 09 01 - Gluten Free - Heaven PDFDocument100 pages2018 09 01 - Gluten Free - Heaven PDFLia VágvölgyiPas encore d'évaluation
- Gluten Free Breads BookDocument49 pagesGluten Free Breads BookPeter Uruel L. Pilar100% (5)
- FarmfreshfareguideDocument13 pagesFarmfreshfareguideapi-276355836Pas encore d'évaluation
- 33 Gluten Free Breakfasts - Gluten-FreeDocument78 pages33 Gluten Free Breakfasts - Gluten-FreeIka Risca100% (2)
- No Sacrifices Cookbook - Entertaining Gluten-FreeDocument37 pagesNo Sacrifices Cookbook - Entertaining Gluten-FreeEllen EmersonPas encore d'évaluation
- Phytates and Phytic AcidDocument8 pagesPhytates and Phytic AcidAdrian StanPas encore d'évaluation
- Easy Gluten Free RecipesDocument90 pagesEasy Gluten Free RecipesBrandon Schmid100% (1)
- PC Cooking With Pulses Web-Ready SpreadsDocument25 pagesPC Cooking With Pulses Web-Ready SpreadsJeffrey PeekoPas encore d'évaluation
- Gluten Free RecipesDocument16 pagesGluten Free Recipessunsetguy70% (10)
- Gluten Free BookletDocument32 pagesGluten Free BookletMaría Julia Ogna Egea100% (8)
- ProbioticsDocument26 pagesProbioticsShnabay DaryaPas encore d'évaluation
- 10 Ways To Avoid The FluDocument1 page10 Ways To Avoid The FluHarperOne (an imprint of HarperCollins)11% (9)
- 4 Week Gluten Free Meal PlanDocument14 pages4 Week Gluten Free Meal Plannicolas0danek67% (3)
- The Health RevolutionDocument214 pagesThe Health RevolutionFisnik Y. Limani0% (1)
- Cookbook For NerdsDocument73 pagesCookbook For NerdsFlowchart Kitchen100% (2)
- GlutenFree Sourdough Ebook PDFDocument207 pagesGlutenFree Sourdough Ebook PDFFábio Barrozo Pinto Fernandes100% (6)
- Kidney Failure:Eat Right To Feel Right On HemodialysisDocument28 pagesKidney Failure:Eat Right To Feel Right On HemodialysisSarah JT100% (2)
- Milk Proteins Good & BadDocument3 pagesMilk Proteins Good & BadJose PalomarPas encore d'évaluation
- Cholesterol Factors Determining Blood Cholesterol LevelsDocument7 pagesCholesterol Factors Determining Blood Cholesterol LevelsAnonymous bKm5eCtPas encore d'évaluation
- Eating Guide For A Low-Oxalate Diet PDFDocument2 pagesEating Guide For A Low-Oxalate Diet PDFAbdelhaiPas encore d'évaluation
- Gluten Free CookingDocument113 pagesGluten Free CookingMark LatterPas encore d'évaluation
- 5 Ways To Turn Any Treat Into A Delicious Healthy RecipeDocument22 pages5 Ways To Turn Any Treat Into A Delicious Healthy Recipealex_grgPas encore d'évaluation
- Basic Macrobiotic Cooking PDFDocument290 pagesBasic Macrobiotic Cooking PDFAntiSpamReg100% (11)
- Boost Your Brainpower A Simplified Approach To The Brain Maker Diet - Jim Stevens PDFDocument43 pagesBoost Your Brainpower A Simplified Approach To The Brain Maker Diet - Jim Stevens PDFcbrcoder100% (4)
- Fake Meat Hoax Aug 31 2019Document27 pagesFake Meat Hoax Aug 31 2019Edz LacsaPas encore d'évaluation
- Gluten Free LivingDocument29 pagesGluten Free Livingapi-366772878Pas encore d'évaluation
- DR Peter Osborne 2021 Warrior Way Cookbook UpdatedDocument18 pagesDR Peter Osborne 2021 Warrior Way Cookbook UpdatedViolet VioletPas encore d'évaluation
- Anticancer LeafletDocument16 pagesAnticancer LeafletJustin100% (1)
- The Cultured Club: Fabulously Funky Fermentation Recipes - Dearbhla ReynoldsDocument6 pagesThe Cultured Club: Fabulously Funky Fermentation Recipes - Dearbhla ReynoldszaxadogyPas encore d'évaluation
- The Autoimmune Fix: How To Stop The Hidden Autoimmune Damage That Keeps You Sick, Fat, and Tired Before It Turns Into Disease - Tom O'BryanDocument4 pagesThe Autoimmune Fix: How To Stop The Hidden Autoimmune Damage That Keeps You Sick, Fat, and Tired Before It Turns Into Disease - Tom O'BryanxehuwumePas encore d'évaluation
- Nutrition and ImmunityDocument40 pagesNutrition and ImmunityTugas HeinzPas encore d'évaluation
- Hardy Fruits For AlbertaDocument13 pagesHardy Fruits For Albertadekaymail0% (1)
- Supergrains by Chrissy FreerDocument11 pagesSupergrains by Chrissy FreerRandom House of Canada0% (2)
- PDF Recipes - Dale's Recipe Book V3Document142 pagesPDF Recipes - Dale's Recipe Book V3ra$hPas encore d'évaluation
- Gluten Free Lifestyle - Best Diet For Gluten Intolerance - Secrets To Excellent Gut HealthD'EverandGluten Free Lifestyle - Best Diet For Gluten Intolerance - Secrets To Excellent Gut HealthPas encore d'évaluation
- Gluten-Free Kids Lunch Break 60 Fuss-Free Delicious, Easy-To-Make, School-Ready Breakfast, Snack, & Lunch RecipesD'EverandGluten-Free Kids Lunch Break 60 Fuss-Free Delicious, Easy-To-Make, School-Ready Breakfast, Snack, & Lunch RecipesPas encore d'évaluation
- My Gut: How to overcome IBS, SIBO and other digestive issuesD'EverandMy Gut: How to overcome IBS, SIBO and other digestive issuesPas encore d'évaluation
- Playoff Game 2Document2 pagesPlayoff Game 2DarrenlellisPas encore d'évaluation
- Game 12Document2 pagesGame 12DarrenlellisPas encore d'évaluation
- Playoff 1Document2 pagesPlayoff 1DarrenlellisPas encore d'évaluation
- 2010RookiePlayoffs 1Document1 page2010RookiePlayoffs 1DarrenlellisPas encore d'évaluation
- Cubs V MarliDocument5 pagesCubs V MarliDarrenlellisPas encore d'évaluation
- Game 13Document2 pagesGame 13DarrenlellisPas encore d'évaluation
- Marli V AstroDocument5 pagesMarli V AstroDarrenlellisPas encore d'évaluation
- Oriol V MarliDocument5 pagesOriol V MarliDarrenlellisPas encore d'évaluation
- Game 10Document2 pagesGame 10DarrenlellisPas encore d'évaluation
- Game 11Document2 pagesGame 11DarrenlellisPas encore d'évaluation
- Game 9Document4 pagesGame 9DarrenlellisPas encore d'évaluation
- Range V Marli-1Document5 pagesRange V Marli-1DarrenlellisPas encore d'évaluation
- Game 8Document2 pagesGame 8DarrenlellisPas encore d'évaluation
- Playoff ScheduleDocument1 pagePlayoff ScheduleDarrenlellisPas encore d'évaluation
- Game 4Document2 pagesGame 4DarrenlellisPas encore d'évaluation
- Game 4Document2 pagesGame 4DarrenlellisPas encore d'évaluation
- Marli V YankeDocument5 pagesMarli V YankeDarrenlellisPas encore d'évaluation
- Game 6Document2 pagesGame 6DarrenlellisPas encore d'évaluation
- Game 5Document2 pagesGame 5DarrenlellisPas encore d'évaluation
- TSSPicture Form 2010Document2 pagesTSSPicture Form 2010DarrenlellisPas encore d'évaluation
- Game 3Document2 pagesGame 3DarrenlellisPas encore d'évaluation
- Marli V IndiaDocument5 pagesMarli V IndiaDarrenlellisPas encore d'évaluation
- Cardi V MarliDocument5 pagesCardi V MarliDarrenlellisPas encore d'évaluation
- Game 2Document2 pagesGame 2DarrenlellisPas encore d'évaluation
- Marli V Reds - 1Document4 pagesMarli V Reds - 1DarrenlellisPas encore d'évaluation
- Game 2Document2 pagesGame 2DarrenlellisPas encore d'évaluation
- 1999, 2003 - Purple Triangles - BrochureDocument32 pages1999, 2003 - Purple Triangles - BrochureMaria Patinha100% (2)
- Entrepreneur: Job/Career InvolvementDocument5 pagesEntrepreneur: Job/Career InvolvementYlaissa GeronimoPas encore d'évaluation
- Head InjuryDocument7 pagesHead InjuryRoshan Ghimire100% (1)
- Institute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationDocument10 pagesInstitute of Actuaries of India: Subject CT3-Probability and Mathematical Statistics May 2008 ExaminationeuticusPas encore d'évaluation
- Spyderco Product Guide - 2016Document154 pagesSpyderco Product Guide - 2016marceudemeloPas encore d'évaluation
- Plastique: Art and EducationDocument7 pagesPlastique: Art and EducationJackStevensonPas encore d'évaluation
- RPT Form 2 2023Document7 pagesRPT Form 2 2023NOREEN BINTI DOASA KPM-GuruPas encore d'évaluation
- Acidity (As Acetic Acid) On Undenatured and Denatured EthanolDocument10 pagesAcidity (As Acetic Acid) On Undenatured and Denatured EthanolVinh NguyenPas encore d'évaluation
- Analysing Worship in The Pentateuch and Its ApplicationDocument12 pagesAnalysing Worship in The Pentateuch and Its ApplicationDaniel Solomon100% (1)
- Ylarde vs. Aquino, GR 33722 (DIGEST)Document1 pageYlarde vs. Aquino, GR 33722 (DIGEST)Lourdes Loren Cruz67% (3)
- Number SystemsDocument165 pagesNumber SystemsapamanPas encore d'évaluation
- Boden 2015 Mass Media Playground of StereotypingDocument16 pagesBoden 2015 Mass Media Playground of StereotypingMiguel CuevaPas encore d'évaluation
- ThesisDocument58 pagesThesisTirtha Roy BiswasPas encore d'évaluation
- (Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFDocument451 pages(Durt, - Christoph - Fuchs, - Thomas - Tewes, - Christian) Embodiment, Enaction, and Culture PDFnlf2205100% (3)
- Nguyễn Thị Ngọc Huyền - 19125516 - Homework 3Document7 pagesNguyễn Thị Ngọc Huyền - 19125516 - Homework 3Nguyễn HuyềnPas encore d'évaluation
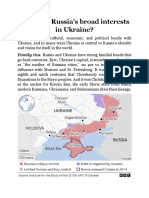
- What Are RussiaDocument3 pagesWhat Are RussiaMuhammad SufyanPas encore d'évaluation
- Adolescent Violence Towards Parents Myths and RealitiesDocument25 pagesAdolescent Violence Towards Parents Myths and RealitiesJoão D C MendonçaPas encore d'évaluation
- Sale Deed Document Rajyalakshmi, 2222222Document3 pagesSale Deed Document Rajyalakshmi, 2222222Madhav Reddy100% (2)
- Tool Stack Template 2013Document15 pagesTool Stack Template 2013strganeshkumarPas encore d'évaluation
- WHO CDS HIV 19.8 EngDocument24 pagesWHO CDS HIV 19.8 EngMaykel MontesPas encore d'évaluation
- International Human Rights LawDocument21 pagesInternational Human Rights LawRea Nica GeronaPas encore d'évaluation
- Openfire XXMPP Server On Windows Server 2012 R2Document9 pagesOpenfire XXMPP Server On Windows Server 2012 R2crobertoPas encore d'évaluation
- AS 1 Pretest TOS S.Y. 2018-2019Document2 pagesAS 1 Pretest TOS S.Y. 2018-2019Whilmark Tican MucaPas encore d'évaluation
- Asset Integrity ManagementDocument5 pagesAsset Integrity ManagementLuis100% (2)
- PED100 Mod2Document3 pagesPED100 Mod2Risa BarritaPas encore d'évaluation
- Scribe FormDocument2 pagesScribe FormsiddharthgamrePas encore d'évaluation
- FreeMarkets: Procurement & Outsourcing StrategiesDocument44 pagesFreeMarkets: Procurement & Outsourcing StrategiesFarhaad MohsinPas encore d'évaluation
- Asset Management PlanDocument160 pagesAsset Management Planbkalatus1100% (1)
- Unit 2 Foundations of CurriculumDocument20 pagesUnit 2 Foundations of CurriculumKainat BatoolPas encore d'évaluation
- Chapter Three: Research MethodologyDocument3 pagesChapter Three: Research MethodologyEng Abdulkadir MahamedPas encore d'évaluation