Vous aimerez peut-être aussi
- THIEME Atlas of Anatomy Head and NeuroanatomyDocument1 pageTHIEME Atlas of Anatomy Head and NeuroanatomyP Venkata Sai ACRPas encore d'évaluation
- Thy-1 Modulates Neurological Cell-Cell and Cell-Matrix Interactions Through Multiple Molecular InteractionsDocument19 pagesThy-1 Modulates Neurological Cell-Cell and Cell-Matrix Interactions Through Multiple Molecular InteractionsdupuytrenPas encore d'évaluation
- Wild-Type Huntingtin Plays A Role in Brain Development and Neuronal SurvivalDocument17 pagesWild-Type Huntingtin Plays A Role in Brain Development and Neuronal SurvivalRealAelixirPas encore d'évaluation
- The Non-Muscle Actinopathy-Associated Mutation E33Document32 pagesThe Non-Muscle Actinopathy-Associated Mutation E33Flavia ChPas encore d'évaluation
- 1 s2.0 S0896627318309024 MainDocument23 pages1 s2.0 S0896627318309024 MainDevonPas encore d'évaluation
- tmpE0F TMPDocument11 pagestmpE0F TMPFrontiersPas encore d'évaluation
- Mutant Huntingtin Impairs Axonal Trafficking in MaDocument16 pagesMutant Huntingtin Impairs Axonal Trafficking in MaAnders AskersrudPas encore d'évaluation
- 9.tucci Et Al 2014Document15 pages9.tucci Et Al 2014MiaPas encore d'évaluation
- HypothalaDocument13 pagesHypothalaijafetPas encore d'évaluation
- Serotonin in Animal Cognition and Behavior: Molecular SciencesDocument23 pagesSerotonin in Animal Cognition and Behavior: Molecular SciencesRifqi Hamdani PasaribuPas encore d'évaluation
- Astrozyten DissertationDocument10 pagesAstrozyten DissertationBuyCheapPapersOnlineCanada100% (1)
- Comparative Gene Expression Analysis of Genital TubercleDocument29 pagesComparative Gene Expression Analysis of Genital TubercleAnonymous rprdjdFMNzPas encore d'évaluation
- Motor Cortical Beta Transients Delay Movement Initiation and Track ErrorsDocument39 pagesMotor Cortical Beta Transients Delay Movement Initiation and Track ErrorsjbonaiutoPas encore d'évaluation
- The Role of 5-HT Systems on Memory and Dysfunctional Memory: Emergent Targets for Memory Formation and Memory AlterationsD'EverandThe Role of 5-HT Systems on Memory and Dysfunctional Memory: Emergent Targets for Memory Formation and Memory AlterationsPas encore d'évaluation
- Jara 2018Document54 pagesJara 2018Torres Pineda OsvaldoPas encore d'évaluation
- Liudmyla Tsyba, Oleksii Nikolaienko, Oleksandr Dergai, Mykola Dergai, Olga Novokhatska, Inessa Skrypkina, Alla RynditchDocument9 pagesLiudmyla Tsyba, Oleksii Nikolaienko, Oleksandr Dergai, Mykola Dergai, Olga Novokhatska, Inessa Skrypkina, Alla RynditchSergeat18BPas encore d'évaluation
- IAPSA - Regression RettDocument13 pagesIAPSA - Regression RettEliana CarolinaPas encore d'évaluation
- Antibody Appears To Attack Cancer Cells, Leaving Other Cells UnscathedDocument13 pagesAntibody Appears To Attack Cancer Cells, Leaving Other Cells UnscathedAnonymous EdgflnjcPas encore d'évaluation
- Ramesh 2018Document11 pagesRamesh 2018Ricardo MedinaPas encore d'évaluation
- DBS HuntingtonDocument10 pagesDBS HuntingtonEdith SteinPas encore d'évaluation
- 18wadhwaetal, 173 178cDocument6 pages18wadhwaetal, 173 178cSurendar KesavanPas encore d'évaluation
- Marcos Et Al., 2018Document17 pagesMarcos Et Al., 2018Constanza FuentesPas encore d'évaluation
- MSR 138Document18 pagesMSR 138kamil mahdiPas encore d'évaluation
- Developmental Analysis of Lingo-1/Lern1 Protein Expression in The Mouse Brain: Interaction of Its Intracellular Domain With Myt1lDocument21 pagesDevelopmental Analysis of Lingo-1/Lern1 Protein Expression in The Mouse Brain: Interaction of Its Intracellular Domain With Myt1lМария СавенкоPas encore d'évaluation
- J Psyneuen 2013 02 002 SEXUALDocument17 pagesJ Psyneuen 2013 02 002 SEXUALIbrahim TaşçioğluPas encore d'évaluation
- Histone Deacetylases and Cancer: ReviewDocument11 pagesHistone Deacetylases and Cancer: ReviewNacido para BendcirPas encore d'évaluation
- Review: Mitochondria: in Sickness and in HealthDocument15 pagesReview: Mitochondria: in Sickness and in HealthPetra JobovaPas encore d'évaluation
- Glia Paper 2015Document22 pagesGlia Paper 2015MelaniePas encore d'évaluation
- DNA Methylation Patterns and Epigenetic Memory: Adrian BirdDocument16 pagesDNA Methylation Patterns and Epigenetic Memory: Adrian BirdAdrian GuzmanPas encore d'évaluation
- InmunohistoquímicaDocument18 pagesInmunohistoquímicaViviana LunaPas encore d'évaluation
- Mielinizacion 2Document12 pagesMielinizacion 2sabadboy 01Pas encore d'évaluation
- Colin-Acetil Transferaza PDFDocument25 pagesColin-Acetil Transferaza PDFMarina AlinaPas encore d'évaluation
- Botulinum Neurotoxins: Mechanism of Action: O. Rossetto, M. Pirazzini, F. Fabris, and C. MontecuccoDocument13 pagesBotulinum Neurotoxins: Mechanism of Action: O. Rossetto, M. Pirazzini, F. Fabris, and C. Montecuccofmmw6qdgzvPas encore d'évaluation
- Rodriguez-Nuevo Et Al-2018Document18 pagesRodriguez-Nuevo Et Al-2018NikoPas encore d'évaluation
- Cell 2010 WooDocument12 pagesCell 2010 WooAdrian GuzmanPas encore d'évaluation
- Epigenetic Eti Old IDocument10 pagesEpigenetic Eti Old IStella IguiniPas encore d'évaluation
- Frontiers in BiologyDocument14 pagesFrontiers in BiologyAkademisyen BirisiPas encore d'évaluation
- JCB 202209062Document21 pagesJCB 202209062Aleksay NesmashnyyPas encore d'évaluation
- Nihms 386408Document25 pagesNihms 386408Carturo VduncanPas encore d'évaluation
- PsychFest - Lipid Droplets in HepatocytesDocument1 pagePsychFest - Lipid Droplets in HepatocytesAj KeefePas encore d'évaluation
- Mykola Dergai, Inessa Skrypkina, Oleksandr Dergai, Liudmyla Tsyba, Olga Novokhatska, Valeriy Filonenko, Lyudmyla Drobot, Alla RynditchDocument10 pagesMykola Dergai, Inessa Skrypkina, Oleksandr Dergai, Liudmyla Tsyba, Olga Novokhatska, Valeriy Filonenko, Lyudmyla Drobot, Alla RynditchSergeat18BPas encore d'évaluation
- Altered Brain Energy Metabolism Related To Astrocytes in Alzheimer's DiseaseDocument33 pagesAltered Brain Energy Metabolism Related To Astrocytes in Alzheimer's DiseaseКолевска МиленаPas encore d'évaluation
- Global Gene Expression Profiling of The Polyamine System in Suicide CompletersDocument11 pagesGlobal Gene Expression Profiling of The Polyamine System in Suicide CompletersSimon NoëlPas encore d'évaluation
- Effect of Cholestasis and NeuroAid Treatment On The ExpressionDocument10 pagesEffect of Cholestasis and NeuroAid Treatment On The ExpressionMohammad Hadi SahebiPas encore d'évaluation
- Dev 146589Document8 pagesDev 146589Zeynep YazıcıoğluPas encore d'évaluation
- Neurotrophic Factors in Alzheimer's Disease: Role of Axonal TransportDocument14 pagesNeurotrophic Factors in Alzheimer's Disease: Role of Axonal Transportaria tristayanthiPas encore d'évaluation
- Journal of Genetics and GenomicsDocument12 pagesJournal of Genetics and Genomicsa lPas encore d'évaluation
- 27 09 2022 MainDocument35 pages27 09 2022 MainPatricia GomesPas encore d'évaluation
- Neurobiology of Disease: A B A A A D C A 1 A B D 1Document12 pagesNeurobiology of Disease: A B A A A D C A 1 A B D 1Duxan Arancibia RadichPas encore d'évaluation
- 2021.04.19.440397v1.full طارقDocument35 pages2021.04.19.440397v1.full طارقTareq aliPas encore d'évaluation
- Activating Mutations of STAT3 - Impact On Human GrowthDocument7 pagesActivating Mutations of STAT3 - Impact On Human Growthmgutierrez.cediePas encore d'évaluation
- Therapeutic Approaches For Inhibition of Protein Aggregation in Huntington's DiseaseDocument9 pagesTherapeutic Approaches For Inhibition of Protein Aggregation in Huntington's DiseaseJorge ElectoPas encore d'évaluation
- M TorDocument6 pagesM TorAhmed NagehPas encore d'évaluation
- Glymphatic System Disruption As A Mediator of Brain - 2018 - Neuroscience - BiobDocument9 pagesGlymphatic System Disruption As A Mediator of Brain - 2018 - Neuroscience - BiobBruno MañonPas encore d'évaluation
- Vip-2010.cytidine Deaminases AIDing DNA DemethylationDocument9 pagesVip-2010.cytidine Deaminases AIDing DNA Demethylationhualin2010Pas encore d'évaluation
- Gabriele Et Al. 2014 - Blood Serotonin Levels in Autism Spectrum DisorderDocument11 pagesGabriele Et Al. 2014 - Blood Serotonin Levels in Autism Spectrum DisorderJuliana JustinoPas encore d'évaluation
- Botulinum Toxin in CancerDocument11 pagesBotulinum Toxin in CancerAlicia Ramirez HernandezPas encore d'évaluation
- Semenza 2016Document35 pagesSemenza 2016winnickimariusz96Pas encore d'évaluation
- Genome Res.-2022-Hirsch-gr.276196.121Document36 pagesGenome Res.-2022-Hirsch-gr.276196.121jaenciPas encore d'évaluation
- Neurobiology of Disease: E.N. Mangano, S. Peters, D. Litteljohn, R. So, C. Bethune, J. Bobyn, M. Clarke, S. HayleyDocument14 pagesNeurobiology of Disease: E.N. Mangano, S. Peters, D. Litteljohn, R. So, C. Bethune, J. Bobyn, M. Clarke, S. HayleyShawn HayleyPas encore d'évaluation
- A Systematic Review of Subjects For PG Medical Entrance ExaminationsDocument995 pagesA Systematic Review of Subjects For PG Medical Entrance ExaminationsRonnie Luzuriaga82% (11)
- LP 1.2 in PhysioBio PsychologyDocument11 pagesLP 1.2 in PhysioBio PsychologyWayne GodioPas encore d'évaluation
- The Nervous System 1ae60 62e99ab3Document1 pageThe Nervous System 1ae60 62e99ab3shamshadPas encore d'évaluation
- 12 Physiology of Autonomic Nervous SystemDocument39 pages12 Physiology of Autonomic Nervous SystemVinod SharmaPas encore d'évaluation
- Report TextDocument5 pagesReport TextJuniorzSunshinersPas encore d'évaluation
- Lesson PlansDocument33 pagesLesson Plansjaclyn71171% (7)
- MIT 9.00 Exam 1 2007 AnswersDocument16 pagesMIT 9.00 Exam 1 2007 AnswersbitternessinmymouthPas encore d'évaluation
- Kuliah PPDS - Cranial NerveDocument68 pagesKuliah PPDS - Cranial Nervederi rivanoPas encore d'évaluation
- Spinal Cord Injury LesionsDocument52 pagesSpinal Cord Injury LesionsbahadurPas encore d'évaluation
- Renal Colic: Roheman, S.Kep, Ners, M.KepDocument33 pagesRenal Colic: Roheman, S.Kep, Ners, M.KeplukmankyubiPas encore d'évaluation
- Medical NeurobiologyDocument682 pagesMedical NeurobiologyMaría CristinaPas encore d'évaluation
- BrainDocument41 pagesBrainWata Regaliza ParongPas encore d'évaluation
- Cerebellum: Anatomy Department Hasanuddin UniversityDocument23 pagesCerebellum: Anatomy Department Hasanuddin Universitynurul rezki fitrianiazisPas encore d'évaluation
- Physiology JOHARIDocument165 pagesPhysiology JOHARIArrya DSPas encore d'évaluation
- Medial Lemniscus Pathway: Ascending Tracts Dorsal ColumnDocument4 pagesMedial Lemniscus Pathway: Ascending Tracts Dorsal ColumnAfrah AbdulPas encore d'évaluation
- Cellular Components 1Document40 pagesCellular Components 1farzadcop1Pas encore d'évaluation
- Anaphy ReviewerDocument9 pagesAnaphy ReviewerPrince Chester CamaliganPas encore d'évaluation
- Physiological Basis of BehaviorDocument35 pagesPhysiological Basis of BehaviorAnna Rhea BurerosPas encore d'évaluation
- Macleod - S - Clinical - Examination - 15th NeuroDocument18 pagesMacleod - S - Clinical - Examination - 15th Neurowxyngtc4n9Pas encore d'évaluation
- 1971 Albus - A Theory of Cerebellar FunctionDocument37 pages1971 Albus - A Theory of Cerebellar FunctionmarkmcwilliamsPas encore d'évaluation
- Lecture 11. Avian Nervous SystemDocument6 pagesLecture 11. Avian Nervous SystemCube MaximPas encore d'évaluation
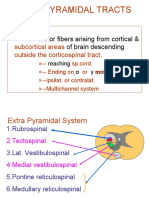
- Extrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingDocument21 pagesExtrapyramidal Tracts: Motor Fibers Arising From Cortical & of Brain DescendingAsfoor gake1Pas encore d'évaluation
- Raeders SyndromeDocument6 pagesRaeders SyndromeSundayperfectPas encore d'évaluation
- Cranial Nerve ExaminationDocument46 pagesCranial Nerve ExaminationKartu KrishnanPas encore d'évaluation
- AP Psych Outline - Chapter 2, Pgs 47-83Document10 pagesAP Psych Outline - Chapter 2, Pgs 47-83Cody DukesPas encore d'évaluation
- Neuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusDocument14 pagesNeuroplasticity: Presented By: Advincula, Arnina Fortus, Jacyrone Pitpit, MarcusCLAIRE DENISSE DEVISPas encore d'évaluation
- Topical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityDocument48 pagesTopical Diagnosis: Department of Anatomy Medical Faculty, Hasanuddin UniversityRey Alwiwikh100% (1)
- Zanki Neuro BoldedDocument25 pagesZanki Neuro Boldedsmian08Pas encore d'évaluation