Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Music TheoryDocument277 pagesMusic TheoryPhilip Mingin100% (5)
- Music TheoryDocument277 pagesMusic TheoryPhilip Mingin100% (5)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Andre Tan's Surgery Notes (Ed 1)Document163 pagesAndre Tan's Surgery Notes (Ed 1)Daniel LimPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Neuro DisordersDocument11 pagesNeuro DisordersPinky CuaresmaPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Cns PathologyDocument18 pagesCns Pathologysunnyorange8Pas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Atls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryDocument55 pagesAtls Important Notes Triage: Ali M. Ahmad Consultant Pediatric SurgeryAndris TapaPas encore d'évaluation
- Atls FlashcardDocument74 pagesAtls Flashcardelnikety100% (5)
- ACLS Provider Manual Supplementary Material: © 2016 American Heart AssociationDocument76 pagesACLS Provider Manual Supplementary Material: © 2016 American Heart AssociationUmbe ChinakaPas encore d'évaluation
- Intensive Care Medicine MCQs Multiple Choice Questions With Explanatory AnswersDocument350 pagesIntensive Care Medicine MCQs Multiple Choice Questions With Explanatory AnswersHiago Sousa59% (17)
- 1917 The Finished Mystery 1918 EditionDocument634 pages1917 The Finished Mystery 1918 EditionLa Bruja del Este100% (1)
- FDARDocument33 pagesFDARMiguelito Galagar Gultiano100% (2)
- Adventure Time Crafts - Finger PuppetsDocument4 pagesAdventure Time Crafts - Finger PuppetsLa Bruja del EstePas encore d'évaluation
- DRUG STUDY - DexamethasoneDocument26 pagesDRUG STUDY - DexamethasoneChristel Santos100% (5)
- DermatologyDocument7 pagesDermatologyLa Bruja del EstePas encore d'évaluation
- Angry Birds PatternDocument1 pageAngry Birds PatternLaura González EstradaPas encore d'évaluation
- Angry Birds PatternDocument1 pageAngry Birds PatternLaura González EstradaPas encore d'évaluation
- CSF RhinorrheaDocument10 pagesCSF RhinorrheaDr-Firas Nayf Al-ThawabiaPas encore d'évaluation
- Nursing Board Exam ReviewerDocument32 pagesNursing Board Exam ReviewerRose Anne Mückl100% (9)
- Cerebral Protection: BY DR - Suneesh Thilak Registrar Anaesthesia Sut Hospital, PattomDocument30 pagesCerebral Protection: BY DR - Suneesh Thilak Registrar Anaesthesia Sut Hospital, PattomsuneeshPas encore d'évaluation
- Standards of Medical Care in Diabetes 2015Document99 pagesStandards of Medical Care in Diabetes 2015Juan Carlos Sánchez Suárez100% (1)
- Abdominal Compartment SyndromeDocument15 pagesAbdominal Compartment SyndromePierinaPas encore d'évaluation
- Omega Light: New Low Level Led TherapiesDocument2 pagesOmega Light: New Low Level Led TherapiesLa Bruja del EstePas encore d'évaluation
- Dangerous Goods HandoutDocument60 pagesDangerous Goods HandoutLa Bruja del Este100% (1)
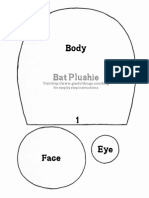
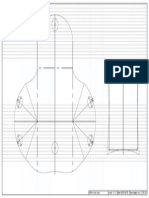
- Bat PatternDocument5 pagesBat PatternLa Bruja del EstePas encore d'évaluation
- Efectos Farmacos Vasoactivos Durante La VentilacionDocument8 pagesEfectos Farmacos Vasoactivos Durante La VentilacionLa Bruja del EstePas encore d'évaluation
- Pediatric Early Warning System Sistema de Alerta TempranaDocument5 pagesPediatric Early Warning System Sistema de Alerta TempranaLa Bruja del EstePas encore d'évaluation
- IOSbasic 9 e 1Document20 pagesIOSbasic 9 e 1La Bruja del EstePas encore d'évaluation
- Avances Choque Hipovolemico PediatricoDocument14 pagesAvances Choque Hipovolemico PediatricoPaty Olán VargasPas encore d'évaluation
- Chapter 14 Pleural DiseaseDocument10 pagesChapter 14 Pleural DiseaseLa Bruja del EstePas encore d'évaluation
- (01/01) Draw:junpei Aoi Date:2015/04/25 Scale: 1:1 Title:coin CaseDocument1 page(01/01) Draw:junpei Aoi Date:2015/04/25 Scale: 1:1 Title:coin CaseLa Bruja del EstePas encore d'évaluation
- 2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionDocument32 pages2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionblueicelandPas encore d'évaluation
- Assassins Creed 3 Hood PART 1Document4 pagesAssassins Creed 3 Hood PART 1Adrian BarilàPas encore d'évaluation
- Wolfplush by Voodoo Tiki-D6pwuknDocument16 pagesWolfplush by Voodoo Tiki-D6pwuknLa Bruja del Este100% (1)
- For Personal Use Only - Not For Commercial Use or ResaleDocument1 pageFor Personal Use Only - Not For Commercial Use or ResaleLa Bruja del EstePas encore d'évaluation
- Vaporeon by Epicvort3x-D7nnzckDocument34 pagesVaporeon by Epicvort3x-D7nnzckLa Bruja del EstePas encore d'évaluation
- GOLD Report 2015Document115 pagesGOLD Report 2015Ana M Gomez APas encore d'évaluation
- BattyDocument2 pagesBattyabdulonnetPas encore d'évaluation
- Simple tips for keeping calm and carrying onDocument1 pageSimple tips for keeping calm and carrying onLa Bruja del EstePas encore d'évaluation
- Poppy Pillow FormDocument4 pagesPoppy Pillow Formcatialx4848Pas encore d'évaluation
- 2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionDocument32 pages2015 GOLD - Pocket Guide To COPD Diagnosis, Management and PreventionblueicelandPas encore d'évaluation
- Subgaleal Haemorrhage Detection and Management in The NewbornDocument9 pagesSubgaleal Haemorrhage Detection and Management in The NewbornVengky UtamiPas encore d'évaluation
- MS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DDocument8 pagesMS Lec Gi and Icp Reviewer - Limon, Adine Jeminah DShawn TejanoPas encore d'évaluation
- Increased Intracranial Pressure (Icp) - Symptoms, Causes, and TreatmentDocument9 pagesIncreased Intracranial Pressure (Icp) - Symptoms, Causes, and TreatmentMarina ShinkoPas encore d'évaluation
- Analisis Asuhan Keperawatandengan Pemberian Oksigenasi Dan Head Up 30 Terhadap Perubahan Haemodinamik Pada Pasien Cedera KepalaDocument6 pagesAnalisis Asuhan Keperawatandengan Pemberian Oksigenasi Dan Head Up 30 Terhadap Perubahan Haemodinamik Pada Pasien Cedera KepalaBoyPas encore d'évaluation
- Understanding Idiopathic Intracranial HypertensionDocument12 pagesUnderstanding Idiopathic Intracranial HypertensionEBPas encore d'évaluation
- Itls 9th Edition Prep Packet Advanced Provider VersionDocument19 pagesItls 9th Edition Prep Packet Advanced Provider VersionUmidagha BaghirzadaPas encore d'évaluation
- PacuDocument45 pagesPacuHeron TitarsolePas encore d'évaluation
- Abdominal Compartment Syndrome in Adults - UpToDateDocument13 pagesAbdominal Compartment Syndrome in Adults - UpToDateMariana PerezPas encore d'évaluation
- Intracranial PressureDocument27 pagesIntracranial PressureAnggaSunaryaPas encore d'évaluation
- Approach To Comatose Child: DR G.VenkateshDocument83 pagesApproach To Comatose Child: DR G.VenkateshG VenkateshPas encore d'évaluation
- Anaesthesia For Neurosurgery-PIIS1472029919302656Document6 pagesAnaesthesia For Neurosurgery-PIIS1472029919302656james Wilson09Pas encore d'évaluation
- World Neurosurgery: X: Teodor Svedung Wettervik, Anders Lew En, Per EnbladDocument13 pagesWorld Neurosurgery: X: Teodor Svedung Wettervik, Anders Lew En, Per EnbladVictor Hugo SilveiraPas encore d'évaluation
- Quiz1 Finals SummerDocument8 pagesQuiz1 Finals SummerMaggay LarsPas encore d'évaluation
- ACS SabistonDocument10 pagesACS Sabistonbocah_britpopPas encore d'évaluation
- Glascow Coma ScaleDocument10 pagesGlascow Coma ScaleJSeasharkPas encore d'évaluation
- Increased Intracranial Pressure (ICP) : Dr. IsazadehfarDocument20 pagesIncreased Intracranial Pressure (ICP) : Dr. Isazadehfarجهاد جواد كاظمPas encore d'évaluation
- Manajemen TIKDocument17 pagesManajemen TIKNathalia Rose Fransisca KarmaPas encore d'évaluation
- Tema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónDocument17 pagesTema 1. - Neurotrauma Aproximación Genral y Estrategias de ResuscitaciónaniadPas encore d'évaluation