Vous aimerez peut-être aussi
- OPP 3 Study Guide Exam 3Document158 pagesOPP 3 Study Guide Exam 3Fazal DalalPas encore d'évaluation
- High Yield OMM ReviewDocument178 pagesHigh Yield OMM ReviewTony ZiherlPas encore d'évaluation
- ANS DrugsDocument2 pagesANS Drugsmed testPas encore d'évaluation
- Sphere: These DiarrheaDocument3 pagesSphere: These Diarrheamed testPas encore d'évaluation
- Sleep stages & blood drinking batsDocument8 pagesSleep stages & blood drinking batsNick100% (1)
- Antipsychotics - AMBOSS PDFDocument7 pagesAntipsychotics - AMBOSS PDFOpio Isaac100% (1)
- Pharmacology Step 1 For USMLEDocument3 pagesPharmacology Step 1 For USMLEraj_1041100% (1)
- OMM Review SheetDocument9 pagesOMM Review SheetSolomon Seth Sallfors100% (2)
- Combank NotesDocument7 pagesCombank NotesVee MendPas encore d'évaluation
- CS Blue Sheet Mnemonics - USMLE Step 2 CSDocument1 pageCS Blue Sheet Mnemonics - USMLE Step 2 CSRafael G. Garcia SanchezPas encore d'évaluation
- Mnemonics Step 1Document4 pagesMnemonics Step 1Raji NaamaniPas encore d'évaluation
- 100 Most Important DrugsDocument13 pages100 Most Important Drugsngopya djiki67% (3)
- Sketchy PharmDocument7 pagesSketchy PharmKacie Jo DillowPas encore d'évaluation
- OMM High YieldDocument25 pagesOMM High YieldHarleen100% (6)
- Medical Student Amnesia USMLE Step 1 - Flash Cards by CueFlashDocument13 pagesMedical Student Amnesia USMLE Step 1 - Flash Cards by CueFlashMuhammad Farhan KhaliqPas encore d'évaluation
- Rapid Infusion for Hypovolemic ShockDocument11 pagesRapid Infusion for Hypovolemic ShocksasghfdgPas encore d'évaluation
- Word AssociationDocument27 pagesWord AssociationMilan Kolovrat100% (1)
- Superficial Back Proximal Insertion Distal Insertion Innervation Blood Supply Function Latissimus DorsiDocument23 pagesSuperficial Back Proximal Insertion Distal Insertion Innervation Blood Supply Function Latissimus Dorsimeyouhere100% (1)
- Platelets and Coagulation SystemDocument5 pagesPlatelets and Coagulation Systemfaithfabulous1_06100% (1)
- Approximate Equivalents:: 0.100 Gmn. 1.00 GMDocument8 pagesApproximate Equivalents:: 0.100 Gmn. 1.00 GMakane ryuPas encore d'évaluation
- LegMusclesDocument78 pagesLegMusclesJoevet T. TadlasPas encore d'évaluation
- Sketchy Pharm Table of ContentsDocument12 pagesSketchy Pharm Table of ContentsMal G100% (1)
- PANCE - Endo Review 2020Document56 pagesPANCE - Endo Review 2020Siam100% (1)
- Pharmayield: Must Know Pharmacology NotesDocument2 pagesPharmayield: Must Know Pharmacology NotesBianca Desiree VergaraPas encore d'évaluation
- OMM CounterstrainDocument11 pagesOMM Counterstrainmasi10Pas encore d'évaluation
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaPas encore d'évaluation
- Comlex Ii & Usmle Ii Cram Sheets - Gastroenterology Vitamins ObesityDocument31 pagesComlex Ii & Usmle Ii Cram Sheets - Gastroenterology Vitamins ObesitySolomon Seth Sallfors100% (1)
- Omm Final TechniquesDocument21 pagesOmm Final TechniquesHeatherCelinaFackelman100% (1)
- Anatomy Shelf Notes Dw9Document200 pagesAnatomy Shelf Notes Dw9Zain ul abedinPas encore d'évaluation
- USMLE Step 1 DrugsDocument36 pagesUSMLE Step 1 DrugscougardiverPas encore d'évaluation
- Ninja On Fleek - Fern Charts MT1Document42 pagesNinja On Fleek - Fern Charts MT1pp100% (1)
- Sports MedicineDocument32 pagesSports Medicinersimranjit100% (1)
- Cardiovascular History: Chest PainDocument5 pagesCardiovascular History: Chest PainTom MallinsonPas encore d'évaluation
- Shock PresentationDocument20 pagesShock Presentationrosalyn sugayPas encore d'évaluation
- List of Medical MnemonicsDocument47 pagesList of Medical MnemonicsSUBHADIPPas encore d'évaluation
- Clinical correlations by Dr. Irfan MirDocument55 pagesClinical correlations by Dr. Irfan MirsammieahemdPas encore d'évaluation
- Comquest NotesDocument58 pagesComquest NotesBhumiShahPas encore d'évaluation
- Brainstem Lesions Trans 2019 PDFDocument8 pagesBrainstem Lesions Trans 2019 PDFVon HippoPas encore d'évaluation
- Diseases of the Pituitary GlandDocument8 pagesDiseases of the Pituitary GlandSheryl Layne Lao-SebrioPas encore d'évaluation
- Second Aid - USMLE MnemonicsDocument21 pagesSecond Aid - USMLE MnemonicsKgerbPas encore d'évaluation
- Combank - Comlex 2 Ce NotesDocument1 pageCombank - Comlex 2 Ce NotesnyecadPas encore d'évaluation
- Antibacterial Drugs SummaryDocument13 pagesAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- Amboss Hemolytic AnemiaDocument16 pagesAmboss Hemolytic AnemiaAhmed Ali100% (2)
- SketchyPath ChecklistDocument1 pageSketchyPath ChecklistFajar Raza100% (1)
- UWorld - Psych Review Charts (From Questions)Document47 pagesUWorld - Psych Review Charts (From Questions)uowhywxuuiragjadchPas encore d'évaluation
- Medical MneumonicsDocument139 pagesMedical MneumonicsdrtpkPas encore d'évaluation
- Kaplan TopicEssentials OMMDocument175 pagesKaplan TopicEssentials OMMNisreen SalamePas encore d'évaluation
- Netter's Anatomy Coloring BookfffffDocument3 pagesNetter's Anatomy Coloring BookfffffAndreea GheorghePas encore d'évaluation
- Back Muscle ChartDocument3 pagesBack Muscle ChartTony Montana100% (1)
- Autonomic Nervous System-1Document46 pagesAutonomic Nervous System-1a-tldPas encore d'évaluation
- Neurologic Conditions 1 SciDocument5 pagesNeurologic Conditions 1 SciEdward De LeonPas encore d'évaluation
- Chapter 31 TrippleDocument6 pagesChapter 31 TripplegeorgefrombaPas encore d'évaluation
- Capobianco Level One ReviewDocument69 pagesCapobianco Level One ReviewkPas encore d'évaluation
- Differentials and Tests Condition Condition: TH THDocument4 pagesDifferentials and Tests Condition Condition: TH THlawlor_jcPas encore d'évaluation
- Evaluation of Lumbar Spine MRIDocument20 pagesEvaluation of Lumbar Spine MRIDharam Pandey100% (2)
- Assessing the Neurologic SystemDocument66 pagesAssessing the Neurologic SystemAngelo EstanislaoPas encore d'évaluation
- Hacks Final FormattedDocument183 pagesHacks Final Formattedbhoj RAJPas encore d'évaluation
- Slide Title Slide Number: Slide 2 Slide 3 Slide 4 Slide 5 Slide 6 Slide 7 Slide 8 Slide 9Document9 pagesSlide Title Slide Number: Slide 2 Slide 3 Slide 4 Slide 5 Slide 6 Slide 7 Slide 8 Slide 9MUHAMMAD AHMAD IBRAHIMPas encore d'évaluation
- Type 2 Diabetes Therapy Options When Metformin is Not ToleratedDocument1 pageType 2 Diabetes Therapy Options When Metformin is Not Toleratedmasi10Pas encore d'évaluation
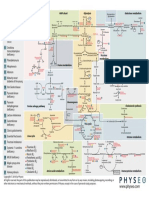
- 6 Biochemistry MapDocument1 page6 Biochemistry Mapmasi10100% (3)
- OMM CounterstrainDocument11 pagesOMM Counterstrainmasi10Pas encore d'évaluation
- GreenLemonDinnerNEW PrintDocument1 pageGreenLemonDinnerNEW Printmasi10Pas encore d'évaluation
- OMM Level 1 ReviewDocument165 pagesOMM Level 1 Reviewmasi10Pas encore d'évaluation
- Acls AlgorithmsDocument8 pagesAcls Algorithmsdydy_7193Pas encore d'évaluation
- Neurologic Exam SkillsDocument11 pagesNeurologic Exam Skillsmasi10Pas encore d'évaluation
- Essential Consumables & EquipmentDocument9 pagesEssential Consumables & EquipmentOverall Clinical CoordinatorPas encore d'évaluation
- New Report About Holyoke Soldiers' HomeDocument10 pagesNew Report About Holyoke Soldiers' HomeMike PlaisancePas encore d'évaluation
- Clinical Pharmacy SyllabusDocument2 pagesClinical Pharmacy Syllabusnemkumar jainPas encore d'évaluation
- Pharmacotherapy Principles for the ElderlyDocument2 pagesPharmacotherapy Principles for the ElderlyStudy ReviewersPas encore d'évaluation
- Rehabbed To Death: PerspectiveDocument2 pagesRehabbed To Death: PerspectiveSandeep SasidharanPas encore d'évaluation
- WorkSafe Reimbursement Rates For Medical Services July 2010Document44 pagesWorkSafe Reimbursement Rates For Medical Services July 2010zurmiePas encore d'évaluation
- Philo 3h NotesDocument5 pagesPhilo 3h Notesapi-3743951100% (3)
- Assignment/ Tugasan - Rehabilitation Geriatric and Palliative CareDocument7 pagesAssignment/ Tugasan - Rehabilitation Geriatric and Palliative CareDamin FyePas encore d'évaluation
- Spending 2012 02Document123 pagesSpending 2012 02Mohammod KhanPas encore d'évaluation
- Core Elements of Evidence-Based Gerontological Nursing PracticeDocument28 pagesCore Elements of Evidence-Based Gerontological Nursing PracticeKaiser Antoja50% (2)
- 【Careworker】Daftar Institusi Penerima Dan Jumlah Calon Kandidat Yang Akan DiterimaDocument2 pages【Careworker】Daftar Institusi Penerima Dan Jumlah Calon Kandidat Yang Akan DiterimaMatahari Putih100% (1)
- Flowsheet For Paediatric Pain AssessmentDocument2 pagesFlowsheet For Paediatric Pain AssessmentschoenePas encore d'évaluation
- Week 1 Part 1Document34 pagesWeek 1 Part 1Melai AvilaPas encore d'évaluation
- DR Robert Stern Declaration in Support of Objection To NFL Concussion Settlement OfferDocument61 pagesDR Robert Stern Declaration in Support of Objection To NFL Concussion Settlement OfferRobert LeePas encore d'évaluation
- Rundown Acara Hari 2 (Peserta)Document2 pagesRundown Acara Hari 2 (Peserta)Ade Perdana SetiawanPas encore d'évaluation
- Psych Micro Teaching - AlzheimersDocument10 pagesPsych Micro Teaching - Alzheimersapi-269113291Pas encore d'évaluation
- Second Year B.SC Nursing Master PlanDocument3 pagesSecond Year B.SC Nursing Master Plancharanjit kaurPas encore d'évaluation
- Late Life and Neurocognitive DisordersDocument24 pagesLate Life and Neurocognitive DisordersJonnaPas encore d'évaluation
- Caregiving 8 Periodical ExamDocument3 pagesCaregiving 8 Periodical ExamLeizette Zuniga Tacang95% (22)
- Dialog Perawat Dan PerawatDocument5 pagesDialog Perawat Dan PerawatnandaPas encore d'évaluation
- Making An Occupied BedDocument2 pagesMaking An Occupied BedJoslyn GrossPas encore d'évaluation
- Norton Risk Assessment ToolDocument4 pagesNorton Risk Assessment ToolFadityo PrihantoroPas encore d'évaluation
- 666 CDR - Scale PDFDocument10 pages666 CDR - Scale PDFIkanpaus Di BlogspotPas encore d'évaluation
- 5589 New Stobhill Hospital CsDocument12 pages5589 New Stobhill Hospital CsNishimaPas encore d'évaluation
- Virtual Dementia Simulation Janedene Guevara 1Document4 pagesVirtual Dementia Simulation Janedene Guevara 1api-485132528Pas encore d'évaluation
- Anp Presentation On GeriatricsDocument114 pagesAnp Presentation On Geriatricsgeetanjali behl100% (3)
- (Panic) Laboratory (Parameter) : PolicyDocument1 page(Panic) Laboratory (Parameter) : Policymy accountPas encore d'évaluation
- Open Letter Calling For New Shelter Beds in TorontoDocument4 pagesOpen Letter Calling For New Shelter Beds in TorontoToronto StarPas encore d'évaluation
- Therapeutic Exercises: Fundamental and Derived PositionsDocument11 pagesTherapeutic Exercises: Fundamental and Derived PositionsAnujGuptaPas encore d'évaluation
- Prime Times July 2018Document24 pagesPrime Times July 2018timesnewspapersPas encore d'évaluation