Vous aimerez peut-être aussi
- SOP - HIV Care Patient Follow-Up ProgrammeDocument23 pagesSOP - HIV Care Patient Follow-Up ProgrammeParwatiPas encore d'évaluation
- 14.6aids Control ProgrammeDocument9 pages14.6aids Control Programmevenkat krishnanPas encore d'évaluation
- Ahmed Linkage PresentationDocument15 pagesAhmed Linkage PresentationKRUSU ISAACPas encore d'évaluation
- Kanyanta .O. Improving Treatment Coverage at Chelston Zonal Hospital of Lusak ProvinceDocument3 pagesKanyanta .O. Improving Treatment Coverage at Chelston Zonal Hospital of Lusak Provincemiyanda mainzaPas encore d'évaluation
- Cdc-Hiv-Adherence Clubs LRC Ebi RetentionDocument4 pagesCdc-Hiv-Adherence Clubs LRC Ebi Retentiontshepoteeman05Pas encore d'évaluation
- 10.1186@s13643-015-0136-x Sistematik ReviewDocument6 pages10.1186@s13643-015-0136-x Sistematik ReviewAnonymous tmw24cW0Pas encore d'évaluation
- Hospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Document18 pagesHospital-Based ACT Intervention To Improve Retention in Care For Persons With HIV - 2021Ashik RahamanPas encore d'évaluation
- Assessing Uptake of National HIV Screening and Testing Guidance-Part 2: Knowledge, Comfort and PracticeDocument9 pagesAssessing Uptake of National HIV Screening and Testing Guidance-Part 2: Knowledge, Comfort and PracticeIrna SulistiyaniPas encore d'évaluation
- A Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativeD'EverandA Clinician’s Guide to HCV Treatment in the Primary Care Setting: A Multimedia eHealth Source™ Educational InitiativePas encore d'évaluation
- Cost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeDocument8 pagesCost Effectiveness of A Care Program For HIV AIDS Patients - 2016 - Value in HeSansa LauraPas encore d'évaluation
- HIV-related Stigma and DiscriminationDocument11 pagesHIV-related Stigma and DiscriminationRey Ann PangilinanPas encore d'évaluation
- Development and Validation of A Sociodemographic ADocument14 pagesDevelopment and Validation of A Sociodemographic AvusPas encore d'évaluation
- Literature Review On Hiv Counselling and TestingDocument4 pagesLiterature Review On Hiv Counselling and Testingwopugemep0h3100% (1)
- Determinants of Facility Readiness For Integration of Family Planning With HIV Testing and Counseling Services: Evidence From The Tanzania Service Provision Assessment Survey, 2014 - 2015Document11 pagesDeterminants of Facility Readiness For Integration of Family Planning With HIV Testing and Counseling Services: Evidence From The Tanzania Service Provision Assessment Survey, 2014 - 2015yuliaPas encore d'évaluation
- Compliance With Quality Guidelines in HIV Anti-Retroviral Treatment Interventions at Kisii Teaching and Referral HospitalDocument9 pagesCompliance With Quality Guidelines in HIV Anti-Retroviral Treatment Interventions at Kisii Teaching and Referral HospitalInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- 2.3 HontelezDocument12 pages2.3 Hontelezallan.manaloto23Pas encore d'évaluation
- DarenoDocument14 pagesDarenoguohong huPas encore d'évaluation
- 2014 - Zurovac - POne - Major Improvements in The Quality of Case Management in KenyaDocument11 pages2014 - Zurovac - POne - Major Improvements in The Quality of Case Management in KenyanomdeplumPas encore d'évaluation
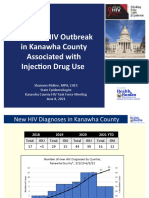
- Update: HIV Outbreak in Kanawha County Associated With Injection Drug UseDocument10 pagesUpdate: HIV Outbreak in Kanawha County Associated With Injection Drug UseJune LefflerPas encore d'évaluation
- Ket ProposalDocument37 pagesKet ProposalEneyew BirhanPas encore d'évaluation
- 2015 Article 1098Document12 pages2015 Article 1098Irenius TenaPas encore d'évaluation
- Nurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMDocument1 pageNurses' Knowledge On Nosocomial Infections Preventive Measures and Its Associated Factors in Ghana A Cross-Sectional Study BMahilhamza55Pas encore d'évaluation
- Initial Health Assessments and HIV Screening Under The Affordable Care ActDocument11 pagesInitial Health Assessments and HIV Screening Under The Affordable Care ActLeon L GayaPas encore d'évaluation
- Patient SatifactionDocument9 pagesPatient SatifactionAndrew CharlesPas encore d'évaluation
- Linkage To HIV Care and Early Retention in Care Rates in The Universal Test-and-Treat Era: A Population-Based Prospective Study in KwaZulu - Natal, South AfricaDocument14 pagesLinkage To HIV Care and Early Retention in Care Rates in The Universal Test-and-Treat Era: A Population-Based Prospective Study in KwaZulu - Natal, South AfricaGlimex Pty LtdPas encore d'évaluation
- Patient Satisfaction and Loyalty To The Private Hospitals in Sana'a, YemenDocument6 pagesPatient Satisfaction and Loyalty To The Private Hospitals in Sana'a, YemenForhad BappyPas encore d'évaluation
- Patient Satisfaction On The Utilization of Traditional and Complementary Medicine Services at Public Hospitals in MalaysiaDocument9 pagesPatient Satisfaction On The Utilization of Traditional and Complementary Medicine Services at Public Hospitals in MalaysiaNurul AnnisaPas encore d'évaluation
- Ndizeye 2018Document8 pagesNdizeye 2018Ajup SafarudinPas encore d'évaluation
- Adherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaDocument7 pagesAdherence Counseling and Reminder Text Messages Improve Uptake of Antiretroviral Therapy in A Tertiary Hospital in NigeriaRiska Resty WasitaPas encore d'évaluation
- Boosting ART Uptake and Retention Among HIV Infected Women and Their InfantsDocument4 pagesBoosting ART Uptake and Retention Among HIV Infected Women and Their InfantsDouglas ChukwuPas encore d'évaluation
- BMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyDocument10 pagesBMC Medicine: Patient-Centred Tuberculosis Treatment Delivery Under Programmatic Conditions in Tanzania: A Cohort StudyNay Lin HtikePas encore d'évaluation
- Tropical Med Int Health - 2015 - Parker - Feasibility and Effectiveness of Two Community Based HIV Testing Models in RuralDocument10 pagesTropical Med Int Health - 2015 - Parker - Feasibility and Effectiveness of Two Community Based HIV Testing Models in Ruralxcr66123Pas encore d'évaluation
- Understanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiDocument34 pagesUnderstanding PHC Reviews and The Nigeria Planning and Implementation Framework - DR Eboreime EjemaiEjemai EboreimePas encore d'évaluation
- A0 No. 2017-0019 Policies and Guidelines in The Conduct of HIV TestingDocument22 pagesA0 No. 2017-0019 Policies and Guidelines in The Conduct of HIV TestingRoderick BalcePas encore d'évaluation
- Economic Evaluation of Point-Of-Care Diagnostic Technologies For Infectious DiseasesDocument7 pagesEconomic Evaluation of Point-Of-Care Diagnostic Technologies For Infectious DiseasesNamita MitraPas encore d'évaluation
- SG Website ExampleDocument21 pagesSG Website ExampleishwaryaPas encore d'évaluation
- Patwa 2019Document10 pagesPatwa 2019Dani HernándezPas encore d'évaluation
- Mapping The Effectiveness of Integrating Mental Health in HIV Programs - A Scoping Review - 2023Document14 pagesMapping The Effectiveness of Integrating Mental Health in HIV Programs - A Scoping Review - 2023Ashik RahamanPas encore d'évaluation
- EthiopiaDocument24 pagesEthiopiaAklilu FelekePas encore d'évaluation
- Provider-Initiated Counselling and Testing PICT AnDocument5 pagesProvider-Initiated Counselling and Testing PICT AnAbebe GedefawPas encore d'évaluation
- Art TerapiDocument7 pagesArt TerapianggaririnPas encore d'évaluation
- Literature Study: Analysis of Factors Causing High Referral Rates inDocument10 pagesLiterature Study: Analysis of Factors Causing High Referral Rates inVeggy LiansyahPas encore d'évaluation
- JC Tuesday 24 AugustDocument9 pagesJC Tuesday 24 AugustsmbawasainiPas encore d'évaluation
- Art 20198412Document19 pagesArt 20198412Nazneen AkhterPas encore d'évaluation
- Vih Ingreso Al Cuidado VihDocument15 pagesVih Ingreso Al Cuidado Vihsamuro625Pas encore d'évaluation
- Behavioural Interventions EngDocument6 pagesBehavioural Interventions EngMatin Ahmad KhanPas encore d'évaluation
- Liaquat University of Sciences: Yusra Bhatti Medical and HealthDocument10 pagesLiaquat University of Sciences: Yusra Bhatti Medical and HealthPharmanic By Ruttaba FatimaPas encore d'évaluation
- Mortality in HIV and TB-NaidooDocument13 pagesMortality in HIV and TB-Naidoodani catriaPas encore d'évaluation
- AI ResearchDocument9 pagesAI ResearchshiringohariiiPas encore d'évaluation
- Evaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictDocument17 pagesEvaluation of The Factors Influencing Adherence To ART in HIVAIDS Patients at Kampala International University Teaching Hospital Bushenyi DistrictKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- DR - Basavaraj.S.Bagli P.G.Scholar Batch 2009-10 Dept of TST, NIUM BangaloreDocument36 pagesDR - Basavaraj.S.Bagli P.G.Scholar Batch 2009-10 Dept of TST, NIUM BangaloreRaj BagliPas encore d'évaluation
- 05b HIV Testing and Counseling (National)Document26 pages05b HIV Testing and Counseling (National)AIDSPhilPas encore d'évaluation
- Early Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsD'EverandEarly Cancer Detection in Primary Care: Are You Aware of New Blood-Based Multi-Cancer Screening ToolsPas encore d'évaluation
- Dental - HIV Intergration - Third Draft - 1Document13 pagesDental - HIV Intergration - Third Draft - 1Emmanuel EjuuPas encore d'évaluation
- Artigo Sobre AidsDocument7 pagesArtigo Sobre AidscamilatututPas encore d'évaluation
- Kumpulan Jurnal InternasionalDocument15 pagesKumpulan Jurnal InternasionalTIKAPas encore d'évaluation
- Contemporary Clinical Trials: SciencedirectDocument10 pagesContemporary Clinical Trials: SciencedirectFristune NewPas encore d'évaluation
- Operational Guidelines Operational Guidelines For ARTfor ART ServicesDocument144 pagesOperational Guidelines Operational Guidelines For ARTfor ART ServicesMd MohiuddinPas encore d'évaluation
- Who Hiv 2003.20Document2 pagesWho Hiv 2003.20kalikPas encore d'évaluation
- Hospital Acquired Infections and Steps To Prevent ThemDocument2 pagesHospital Acquired Infections and Steps To Prevent ThemAbhisek SwainPas encore d'évaluation
- Nutritional Contribution of Mid-Day Meal (MDM) As Per Quantity Norms at Upper Primary Classes in DelhiDocument17 pagesNutritional Contribution of Mid-Day Meal (MDM) As Per Quantity Norms at Upper Primary Classes in DelhiJASH MATHEWPas encore d'évaluation
- Ijsrp p5819 PDFDocument4 pagesIjsrp p5819 PDFJASH MATHEWPas encore d'évaluation
- Biometric Encryption: E-Commerce Security Using Cryptography TechniquesDocument8 pagesBiometric Encryption: E-Commerce Security Using Cryptography TechniquesJASH MATHEWPas encore d'évaluation
- Factors Associated With The Uptake of Cervical Cancer Screening Among Married Women in Udagangoda Grama Niladhari Division, Rathnapura District, Sri LankaDocument4 pagesFactors Associated With The Uptake of Cervical Cancer Screening Among Married Women in Udagangoda Grama Niladhari Division, Rathnapura District, Sri LankaJASH MATHEWPas encore d'évaluation
- Ijsrp p5820 PDFDocument7 pagesIjsrp p5820 PDFJASH MATHEWPas encore d'évaluation
- Ijsrp p5818 PDFDocument5 pagesIjsrp p5818 PDFJASH MATHEWPas encore d'évaluation
- Ijsrp p5816 PDFDocument8 pagesIjsrp p5816 PDFJASH MATHEWPas encore d'évaluation
- The Role of Information and Communication Technology (ICT) and Early Warning System in School Security Based System in North Eastern NigeriaDocument5 pagesThe Role of Information and Communication Technology (ICT) and Early Warning System in School Security Based System in North Eastern NigeriaJASH MATHEWPas encore d'évaluation
- Advertisement Analysis: Syntactic Devices in English MagazinesDocument5 pagesAdvertisement Analysis: Syntactic Devices in English MagazinesJASH MATHEWPas encore d'évaluation
- Factors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiDocument5 pagesFactors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiJASH MATHEWPas encore d'évaluation
- Synthesis and Characterization of Ɣ-Fe 2 O 3 Nanoparticles Photo Anode by Novel Method For Dye Sensitized Solar CellDocument6 pagesSynthesis and Characterization of Ɣ-Fe 2 O 3 Nanoparticles Photo Anode by Novel Method For Dye Sensitized Solar CellJASH MATHEWPas encore d'évaluation
- F - DERIVATIONS ON BP-ALGEBRASDocument11 pagesF - DERIVATIONS ON BP-ALGEBRASJASH MATHEWPas encore d'évaluation
- Factors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiDocument5 pagesFactors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiJASH MATHEWPas encore d'évaluation
- Linkage Between Water, Sanitation and Health Outcomes:An Empirical Analysis of Indian StatesDocument10 pagesLinkage Between Water, Sanitation and Health Outcomes:An Empirical Analysis of Indian StatesJASH MATHEWPas encore d'évaluation
- Assessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityDocument5 pagesAssessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityJASH MATHEWPas encore d'évaluation
- Analysis of Poverty Level Fishermen Community Post Tsunami in Aceh, IndonesiaDocument7 pagesAnalysis of Poverty Level Fishermen Community Post Tsunami in Aceh, IndonesiaJASH MATHEWPas encore d'évaluation
- Comparative Study of Two Beta - Lactamase Test Methods in Five Different Microorganisms Isolated From Azadi Hospital in Kirkuk, IraqDocument4 pagesComparative Study of Two Beta - Lactamase Test Methods in Five Different Microorganisms Isolated From Azadi Hospital in Kirkuk, IraqJASH MATHEWPas encore d'évaluation
- Combining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaDocument13 pagesCombining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaJASH MATHEWPas encore d'évaluation
- Strategy To Enhance Company's Excellent Performance Case Study: PT Sakalaguna SemestaDocument8 pagesStrategy To Enhance Company's Excellent Performance Case Study: PT Sakalaguna SemestaJASH MATHEWPas encore d'évaluation
- Engaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceDocument3 pagesEngaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceJASH MATHEWPas encore d'évaluation
- Molecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaDocument7 pagesMolecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaJASH MATHEWPas encore d'évaluation
- Analysis of Effects of Macroeconomic Variables Against Return On Agriculture StocksDocument8 pagesAnalysis of Effects of Macroeconomic Variables Against Return On Agriculture StocksJASH MATHEWPas encore d'évaluation
- The Shift of Focalization in James Joyce's UlyssesDocument7 pagesThe Shift of Focalization in James Joyce's UlyssesJASH MATHEWPas encore d'évaluation
- Effect of Marketing Communications, Brand Equity, Brand Awareness Attitudes and Decision of Customers PT. Mortgage in South SulawesiDocument8 pagesEffect of Marketing Communications, Brand Equity, Brand Awareness Attitudes and Decision of Customers PT. Mortgage in South SulawesiJASH MATHEWPas encore d'évaluation
- Analysis of Wage and Labor Productivity in The Hospitality IndustryDocument9 pagesAnalysis of Wage and Labor Productivity in The Hospitality IndustryJASH MATHEWPas encore d'évaluation
- Value Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionDocument5 pagesValue Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionJASH MATHEWPas encore d'évaluation
- Environmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaDocument8 pagesEnvironmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaJASH MATHEWPas encore d'évaluation
- Historical Landscape Quality Assessment On Priority Area of Banda Aceh Heritage City, Aceh ProvinceDocument5 pagesHistorical Landscape Quality Assessment On Priority Area of Banda Aceh Heritage City, Aceh ProvinceJASH MATHEWPas encore d'évaluation
- An Adaptive Study of Symbolic Cultural Items Used at The Nchaka Festival in Ogbaland For Textile Design of IdentityDocument16 pagesAn Adaptive Study of Symbolic Cultural Items Used at The Nchaka Festival in Ogbaland For Textile Design of IdentityJASH MATHEWPas encore d'évaluation
- Hegemonic Masculinity and Oppression of Women in CavedwellerDocument6 pagesHegemonic Masculinity and Oppression of Women in CavedwellerJASH MATHEWPas encore d'évaluation
- Writing Assignment 2Document3 pagesWriting Assignment 2api-585262375Pas encore d'évaluation
- Urinary Incontinence in Women A ReviewDocument13 pagesUrinary Incontinence in Women A ReviewJordha HeryndraPas encore d'évaluation
- Salud Familiar - APS y Seguridad Social: Marco Aurelio Sosa GiraldoDocument17 pagesSalud Familiar - APS y Seguridad Social: Marco Aurelio Sosa GiraldoOsomolarPas encore d'évaluation
- AML-Excercise Week 5 (Reviandi Ramadhan)Document5 pagesAML-Excercise Week 5 (Reviandi Ramadhan)Reviandi RamadhanPas encore d'évaluation
- Assessment:: Assignment (Submit Your Answers at Edmodo Assignment Section)Document4 pagesAssessment:: Assignment (Submit Your Answers at Edmodo Assignment Section)Lara BuragayPas encore d'évaluation
- Dissertation Topics of PG Degree Mdms Submitted For The Academic Year 2018-19-2019 20 and 2020 21Document227 pagesDissertation Topics of PG Degree Mdms Submitted For The Academic Year 2018-19-2019 20 and 2020 21Asra QuadriPas encore d'évaluation
- Journal of Hand Surgery Global OnlineDocument5 pagesJournal of Hand Surgery Global OnlineMohammed Shuaib AhmedPas encore d'évaluation
- Laboratory Quality Control Based Risk ManagementDocument12 pagesLaboratory Quality Control Based Risk ManagementPedro C. Jardon0% (1)
- FARMAKOEPIDEMIOLOGIDocument11 pagesFARMAKOEPIDEMIOLOGIAmirahPas encore d'évaluation
- General Gynaecology:, Leo Francis AquilizanDocument15 pagesGeneral Gynaecology:, Leo Francis AquilizanesjayemPas encore d'évaluation
- Chief Executive Officer in Brentwood TN Resume Gary FergusonDocument3 pagesChief Executive Officer in Brentwood TN Resume Gary FergusonGaryFerguson1Pas encore d'évaluation
- Research Proposal For NurseDocument44 pagesResearch Proposal For Nursefiraolab5Pas encore d'évaluation
- Records in Family Health Nursing PracticeDocument3 pagesRecords in Family Health Nursing PracticeSophia Nicole AranasPas encore d'évaluation
- Morbidity and Mortality Among The Motor Vehicle Accident PatientsDocument1 pageMorbidity and Mortality Among The Motor Vehicle Accident Patientssmoto1kPas encore d'évaluation
- Introduction To JubileeDocument117 pagesIntroduction To Jubileeangela gnanaduraiPas encore d'évaluation
- Ruli, Novan - IcdDocument45 pagesRuli, Novan - IcdruliamriPas encore d'évaluation
- HSA 6004101-008-17-03 - 43 FSN - RedactedDocument16 pagesHSA 6004101-008-17-03 - 43 FSN - RedactedF CPPas encore d'évaluation
- Medicare HMO PPO Pharmacy Directory enDocument287 pagesMedicare HMO PPO Pharmacy Directory enUlyssesm90100% (1)
- ACC 2023 ResumenDocument7 pagesACC 2023 ResumenJuan Carlos FloresPas encore d'évaluation
- Foreign Literature FinalsDocument14 pagesForeign Literature FinalsAnghel CruzPas encore d'évaluation
- NSWH RequisitionPD CAM16931Document5 pagesNSWH RequisitionPD CAM16931ddddPas encore d'évaluation
- Deployment Program/ Project Application FormDocument1 pageDeployment Program/ Project Application FormCrystal Ann Monsale TadiamonPas encore d'évaluation
- Improving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamDocument9 pagesImproving Caregivers' Perceptions Regarding Patient Goals of Care/End-of-Life Issues For The Multidisciplinary Critical Care TeamSERGIO ANDRES CESPEDES GUERREROPas encore d'évaluation
- Hospitalisation Claim Form: Borang Tuntutan HospitalDocument2 pagesHospitalisation Claim Form: Borang Tuntutan HospitalMohd Azizee Bin SukorPas encore d'évaluation
- William Charney - Handbook of Modern Hospital Safety, Second Edition (2009, CRC Press) PDFDocument1 174 pagesWilliam Charney - Handbook of Modern Hospital Safety, Second Edition (2009, CRC Press) PDFmayaraPas encore d'évaluation
- Endoftalmitis EndogenaDocument1 pageEndoftalmitis EndogenaAlexander Fabián Rodríguez DíazPas encore d'évaluation
- IDCRP Brown Bag Presentation - CRF - 26feb2015Document33 pagesIDCRP Brown Bag Presentation - CRF - 26feb2015shivam singhPas encore d'évaluation
- Nursing Assignment Sample On Case Study On DementiaDocument12 pagesNursing Assignment Sample On Case Study On DementiaAssignment Essay Help100% (1)
- Acetaminophen and Ibuprofen in The Treatment of Pediatric Fever A Narrative ReviewDocument14 pagesAcetaminophen and Ibuprofen in The Treatment of Pediatric Fever A Narrative ReviewI Made AryanaPas encore d'évaluation
- Layout Puskesmas Tempuran Kab. Magelang: Lantai 1Document2 pagesLayout Puskesmas Tempuran Kab. Magelang: Lantai 1Anugrah Aji AnuPas encore d'évaluation