Vous aimerez peut-être aussi
- Analysis of Colorectal Diseases in Southern ThailandDocument5 pagesAnalysis of Colorectal Diseases in Southern ThailandAlfeus GradyPas encore d'évaluation
- Bone Metastases From Thyroid Carcinoma of Follicular Origin A Single Institutional ExperienceDocument6 pagesBone Metastases From Thyroid Carcinoma of Follicular Origin A Single Institutional ExperienceChavdarPas encore d'évaluation
- Epid of Pancreatic CancerDocument2 pagesEpid of Pancreatic CancerHananya ManroePas encore d'évaluation
- Cancer - 2010 - Italiano - Trends in Survival For Patients With Metastatic Soft Tissue SarcomaDocument6 pagesCancer - 2010 - Italiano - Trends in Survival For Patients With Metastatic Soft Tissue SarcomaAna LimeiraPas encore d'évaluation
- Six-Year Study of Colorectal Carcinoma at a Tertiary Hospital in SindhDocument3 pagesSix-Year Study of Colorectal Carcinoma at a Tertiary Hospital in SindhShahimulk KhattakPas encore d'évaluation
- 11 NisarDocument4 pages11 NisarAlfeus GradyPas encore d'évaluation
- Cummings Et Al-2014-The Journal of PathologyDocument9 pagesCummings Et Al-2014-The Journal of Pathologyalicia1990Pas encore d'évaluation
- Koko's Project 2 Submitted WorkDocument50 pagesKoko's Project 2 Submitted WorkNlemorusa PaschalinePas encore d'évaluation
- Quality of Life of Colorectal Cancer Patients A Literature ReviewDocument6 pagesQuality of Life of Colorectal Cancer Patients A Literature Reviewddyuss90Pas encore d'évaluation
- Colorectal CancerDocument14 pagesColorectal Cancershaqtim100% (2)
- Symptom Management in Hepatocellular Carcinoma: Virginia Chih-Yi Sun, RN, MSN, Anp, and Linda Sarna, RN, DNSC, Faan, AocnDocument9 pagesSymptom Management in Hepatocellular Carcinoma: Virginia Chih-Yi Sun, RN, MSN, Anp, and Linda Sarna, RN, DNSC, Faan, AocnElga Rahadian ArsyahPas encore d'évaluation
- Epidemiology and Molecular Pathology of Gallbladder CancerDocument16 pagesEpidemiology and Molecular Pathology of Gallbladder CancerJavaid MeoPas encore d'évaluation
- Human Germ Cell Tumors Are Developmental Cancers: Impact of Epigenetics On Pathobiology and ClinicDocument28 pagesHuman Germ Cell Tumors Are Developmental Cancers: Impact of Epigenetics On Pathobiology and Clinicarcobaleno589Pas encore d'évaluation
- Principios de OncologiaDocument14 pagesPrincipios de Oncologiaangie18Pas encore d'évaluation
- Philippine Cancer Factsand EstimatesDocument88 pagesPhilippine Cancer Factsand EstimatesCamille Dawne FaminialPas encore d'évaluation
- Overal Survival of Filipinos With Head and Neck SCCADocument6 pagesOveral Survival of Filipinos With Head and Neck SCCAPrincess B. MaristelaPas encore d'évaluation
- Bluethmann2016 PDFDocument9 pagesBluethmann2016 PDFramangPas encore d'évaluation
- Epidem Cancer ColorectalDocument5 pagesEpidem Cancer ColorectalAna MîndrilăPas encore d'évaluation
- Colon Cancer Clinical Macroscopic and MiDocument10 pagesColon Cancer Clinical Macroscopic and MiElena CaterevPas encore d'évaluation
- Filipou - 2016Document4 pagesFilipou - 2016TurboPas encore d'évaluation
- Jurnal CarisoprodolDocument9 pagesJurnal CarisoprodolTegarrachman23Pas encore d'évaluation
- (International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastDocument5 pages(International Journal of Cancer Vol. 77 Iss. 5) Milena Sant - Riccardo Capocaccia - Arduino Verdecchia - Jacques Es - Survival of Women With BreastTulioPas encore d'évaluation
- Metastasis Patterns and PrognoDocument17 pagesMetastasis Patterns and Prognosatria divaPas encore d'évaluation
- Tradução 3Document12 pagesTradução 3Ana AlinePas encore d'évaluation
- Ovarian Sertoli-Leydig Cell Tumors Epidemiological Clinical and Prognostic FactorsDocument9 pagesOvarian Sertoli-Leydig Cell Tumors Epidemiological Clinical and Prognostic FactorsJosé LuisPas encore d'évaluation
- Arndt Et Al 2008Document8 pagesArndt Et Al 2008chatsashPas encore d'évaluation
- Cancer Prevention and Screening of Older Adults: Quratulain Tariq DPTM-F15-075Document7 pagesCancer Prevention and Screening of Older Adults: Quratulain Tariq DPTM-F15-075Hafiz Shahid1Pas encore d'évaluation
- Chole JournalDocument9 pagesChole JournalShaira TanPas encore d'évaluation
- TaiwanDocument11 pagesTaiwanbin linPas encore d'évaluation
- Lectura 1 PDFDocument5 pagesLectura 1 PDFCarmen Castillo RequenaPas encore d'évaluation
- Esophageal Cancer Global TrendsDocument12 pagesEsophageal Cancer Global TrendsResidentes CirugíaPas encore d'évaluation
- Poorer Survival Outcomes For Male Breast Cancer Compared With Female Breast Cancer May Be Attributable To In-Stage MigrationDocument9 pagesPoorer Survival Outcomes For Male Breast Cancer Compared With Female Breast Cancer May Be Attributable To In-Stage MigrationabcdshPas encore d'évaluation
- 1749-7922-6-37 - SalinDocument5 pages1749-7922-6-37 - SalinAnonymous InJS6aYZPas encore d'évaluation
- Krukenberg Tumors of Gastric Origin Versus Colorectal OriginDocument8 pagesKrukenberg Tumors of Gastric Origin Versus Colorectal OriginAnandhika DwijayaPas encore d'évaluation
- DaskivichAnnalsManuscript 1Document27 pagesDaskivichAnnalsManuscript 1Southern California Public RadioPas encore d'évaluation
- Risk-adjusted 30-day mortality rates after colorectal cancer surgery in EnglandDocument9 pagesRisk-adjusted 30-day mortality rates after colorectal cancer surgery in England568563Pas encore d'évaluation
- Canine Mammary Tumors in Santos, Brazil: Clinicopathological and Survival ProfileDocument11 pagesCanine Mammary Tumors in Santos, Brazil: Clinicopathological and Survival ProfileAdelaide Elias MacomePas encore d'évaluation
- 03 - Dustin e Hullihop Epidemiologi Kanker Esofagus JurnalDocument12 pages03 - Dustin e Hullihop Epidemiologi Kanker Esofagus JurnalNatalindah Jokiem Woecandra T. D.Pas encore d'évaluation
- Thyroid Disorders: Evaluation and Management of Thyroid NodulesDocument13 pagesThyroid Disorders: Evaluation and Management of Thyroid NodulesГулпе АлексейPas encore d'évaluation
- Clinical Practice GuidelinesDocument9 pagesClinical Practice GuidelinesAhmad13 RizzqiPas encore d'évaluation
- 1 s2.0 S2405844020304485 MainDocument5 pages1 s2.0 S2405844020304485 MainSome LaPas encore d'évaluation
- Cancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofDocument9 pagesCancer - 2014 - Hallet - Exploring The Rising Incidence of Neuroendocrine Tumors A Population Based Analysis ofRepositorioPas encore d'évaluation
- Sun 等。 - 2018 - Age-dependent difference in impact of fertility pr的副本Document10 pagesSun 等。 - 2018 - Age-dependent difference in impact of fertility pr的副本Jing WangPas encore d'évaluation
- Case Control Obesity and Kidney Cancer1 PDFDocument8 pagesCase Control Obesity and Kidney Cancer1 PDFPatricia Andrea Acevedo ArancibiaPas encore d'évaluation
- ThyroidDocument12 pagesThyroidHendra HermawanPas encore d'évaluation
- Biliary Tract CancerDocument10 pagesBiliary Tract CancerNovitta SariPas encore d'évaluation
- Thyroid Ca MortalityDocument9 pagesThyroid Ca MortalityMade RusmanaPas encore d'évaluation
- Case Study StrokeDocument40 pagesCase Study Strokeymonn100% (1)
- International Incidence and Mortality Trends of Liver Cancer: A Global ProfileDocument9 pagesInternational Incidence and Mortality Trends of Liver Cancer: A Global ProfileNovita ApramadhaPas encore d'évaluation
- Pet ThyroidsDocument21 pagesPet ThyroidsdrmolinammPas encore d'évaluation
- Apakah Follow-Up Lengkap Dan Cukup Lama/ Sufficiently Long and Complete?Document12 pagesApakah Follow-Up Lengkap Dan Cukup Lama/ Sufficiently Long and Complete?Annisa KartikasariPas encore d'évaluation
- Ijbc2020 1963814Document6 pagesIjbc2020 1963814Kurnia AlkatiriPas encore d'évaluation
- Clinical Characteristics of Renal Cancer in MalaysiaDocument4 pagesClinical Characteristics of Renal Cancer in MalaysiaIman ShirazPas encore d'évaluation
- SEER MRCC - ASCO GU 2016 Poster - RaoDocument1 pageSEER MRCC - ASCO GU 2016 Poster - Raoarpit_aiimsPas encore d'évaluation
- PCa 20 EU Prostate Cancer IncidenceDocument15 pagesPCa 20 EU Prostate Cancer IncidenceShuang LiPas encore d'évaluation
- Clinical Outcomes and Mortality in Elderly Peritoneal Dialysis PatientsDocument6 pagesClinical Outcomes and Mortality in Elderly Peritoneal Dialysis PatientsbayuPas encore d'évaluation
- Cancer ColorectalDocument13 pagesCancer ColorectalSihuar Fernando Abarca Lozano100% (1)
- Ax1 BSP FinalDocument18 pagesAx1 BSP FinalSofia Krylova-SmithPas encore d'évaluation
- A Prediction Rule For Risk Stratification of Incidentally Discovered Gallstones: Results From A Large Cohort StudyDocument13 pagesA Prediction Rule For Risk Stratification of Incidentally Discovered Gallstones: Results From A Large Cohort StudyvictorPas encore d'évaluation
- Upper Tract Urothelial CarcinomaD'EverandUpper Tract Urothelial CarcinomaShahrokh F. ShariatPas encore d'évaluation
- Breast Cancer Review ArticleDocument1 pageBreast Cancer Review ArticleNazim ThakranPas encore d'évaluation
- WomenAndChemicals PublicationIWD2016Document66 pagesWomenAndChemicals PublicationIWD2016oc haPas encore d'évaluation
- Adenomyoepithelioma of The Breast: A Brief Diagnostic ReviewDocument5 pagesAdenomyoepithelioma of The Breast: A Brief Diagnostic ReviewSFCHIKIPas encore d'évaluation
- Breast - Dr. HammouriDocument12 pagesBreast - Dr. HammouriMohammad PropensityPas encore d'évaluation
- Healthmedicinet I 2016 12Document361 pagesHealthmedicinet I 2016 12tuni santePas encore d'évaluation
- Prime Times July 2018Document24 pagesPrime Times July 2018timesnewspapersPas encore d'évaluation
- Full Dataset of Papers FormattedDocument234 pagesFull Dataset of Papers FormattedoafsPas encore d'évaluation
- Phyllodes Tumors of The Breast: Natural History, Diagnosis, and TreatmentDocument7 pagesPhyllodes Tumors of The Breast: Natural History, Diagnosis, and TreatmentFrancis BillanesPas encore d'évaluation
- Clinical Oncology Assgn RT Mono BreastDocument9 pagesClinical Oncology Assgn RT Mono Breastapi-511386954Pas encore d'évaluation
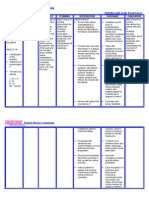
- NURSING CARE PLAN - Breast CancerDocument2 pagesNURSING CARE PLAN - Breast Cancerderic100% (3)
- Breast Self Examination 1Document22 pagesBreast Self Examination 1Juviely PremacioPas encore d'évaluation
- Breast Cancer Staging SystemDocument4 pagesBreast Cancer Staging SystemGabriella PatriciaPas encore d'évaluation
- Literature Review Breast Self Examination ResearchDocument7 pagesLiterature Review Breast Self Examination ResearchaflsigakfPas encore d'évaluation
- 2013-Oncology New QuestionsDocument5 pages2013-Oncology New QuestionsHarley Justiniani Dela CruzPas encore d'évaluation
- MRM Breast Cancer Clinical DiscussionDocument3 pagesMRM Breast Cancer Clinical DiscussionGlare RhaynePas encore d'évaluation
- GS Oral SDSDocument108 pagesGS Oral SDSrobhopp67% (3)
- Oncologic NursingDocument132 pagesOncologic Nursingɹǝʍdןnos100% (10)
- 12.4 Female Reproductive DiseasesDocument20 pages12.4 Female Reproductive Diseasessanat kr pratiharPas encore d'évaluation
- Rating The Risk Factors For Breast Cancer: ReviewDocument9 pagesRating The Risk Factors For Breast Cancer: ReviewPratamasari InsaniPas encore d'évaluation
- Breast Cancer Risk Checklist by DenseBreast-infoDocument4 pagesBreast Cancer Risk Checklist by DenseBreast-infoDense Breast Info IncPas encore d'évaluation
- 5-Febtelegram2019 Correct by New GroupDocument24 pages5-Febtelegram2019 Correct by New GroupFammo MoiduPas encore d'évaluation
- Ductal Carcinoma in SituDocument13 pagesDuctal Carcinoma in SitudrkrsticPas encore d'évaluation
- Pathology - 24 Breast PathologyDocument9 pagesPathology - 24 Breast PathologyNicole WilliamPas encore d'évaluation
- Tommy Emmanuel-Pink PantherDocument5 pagesTommy Emmanuel-Pink PantherP ElstrodtPas encore d'évaluation
- Fungi & Cancer TherapyDocument18 pagesFungi & Cancer TherapyLynn McdonaldPas encore d'évaluation
- The Breast: AnatomyDocument3 pagesThe Breast: AnatomyRyan James Lorenzo Miguel50% (2)
- STUDENT COPY Assessment of Breast and AxillaeDocument57 pagesSTUDENT COPY Assessment of Breast and AxillaeRosette Malenab de AsisPas encore d'évaluation
- CARE Newsletter - July 2012Document12 pagesCARE Newsletter - July 2012Mike RalstonPas encore d'évaluation
- Oncologic Principles in Breast ReconstructionDocument13 pagesOncologic Principles in Breast ReconstructionJose Mauricio Suarez BecerraPas encore d'évaluation
- HalluDocument180 pagesHalluNajib ZulkifliPas encore d'évaluation