Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- 1 The Basics 1Document19 pages1 The Basics 11202blackPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Theologus Autodidact Us of Ibn Al-NafisDocument77 pagesTheologus Autodidact Us of Ibn Al-NafisMujahid Asaadullah Abdullah100% (2)
- Fatal Respiratory Failure During A "Technical" Rebreather Dive at Extreme PressureDocument6 pagesFatal Respiratory Failure During A "Technical" Rebreather Dive at Extreme Pressuretonylee24Pas encore d'évaluation
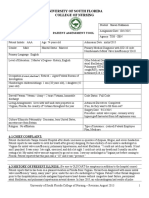
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDocument4 pagesPediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318Pas encore d'évaluation
- Picu WorksheetDocument7 pagesPicu Worksheetapi-324566318Pas encore d'évaluation
- Nicu Worksheet CompletedDocument3 pagesNicu Worksheet Completedapi-324566318Pas encore d'évaluation
- Pat 2 - Semester 2Document27 pagesPat 2 - Semester 2api-324566318Pas encore d'évaluation
- Portfolio-Goals PaperDocument2 pagesPortfolio-Goals Paperapi-324566318Pas encore d'évaluation
- Pat 1 Semester 2 TGH SBN Hekkanen ShawnDocument23 pagesPat 1 Semester 2 TGH SBN Hekkanen Shawnapi-324566318Pas encore d'évaluation
- Pediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467LDocument4 pagesPediatric Nursing Process Worksheet: USF College of Nursing: NUR 4467Lapi-324566318Pas encore d'évaluation
- Final Draft Discussion Board 3-EthicsDocument3 pagesFinal Draft Discussion Board 3-Ethicsapi-324566318Pas encore d'évaluation
- 043 Eco Star Oxy BriteDocument2 pages043 Eco Star Oxy Briteeng20072007Pas encore d'évaluation
- Indian Institute of Technology Delhi: Hauz Khas, New Delhi - 110 016. Website: WWW - Iitd.ac - inDocument6 pagesIndian Institute of Technology Delhi: Hauz Khas, New Delhi - 110 016. Website: WWW - Iitd.ac - inRajesh KumarPas encore d'évaluation
- Health Emergency Kits Training 2019 PDFDocument33 pagesHealth Emergency Kits Training 2019 PDFrema_rhere95Pas encore d'évaluation
- ACT Guide-Final PDFDocument25 pagesACT Guide-Final PDFedw68Pas encore d'évaluation
- Ich GCP: HistoryDocument57 pagesIch GCP: HistoryChandrashekhar Singh100% (1)
- CPCSEADocument27 pagesCPCSEAobaidPas encore d'évaluation
- Animal Physiology Biology CollectionDocument89 pagesAnimal Physiology Biology CollectionAlex Mugurel JitaruPas encore d'évaluation
- Triclosan USP..Document2 pagesTriclosan USP..Arun Kumar PandeyPas encore d'évaluation
- Chinese Face ReadingDocument6 pagesChinese Face ReadingGloria GarzaPas encore d'évaluation
- Root Canal Irrigants in Primary TeethDocument6 pagesRoot Canal Irrigants in Primary TeethsyedPas encore d'évaluation
- Grass Jelly On Glycemic ControlDocument11 pagesGrass Jelly On Glycemic ControlAnanta ArioPas encore d'évaluation
- Digestive System - Part 1Document20 pagesDigestive System - Part 1AndrewPas encore d'évaluation
- Daftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan MenyusuiDocument10 pagesDaftar Obat Yang Dianjurkan Untuk Ibu Hamil Dan Menyusuisunar4deris5413Pas encore d'évaluation
- 00 Biomedical Waste InterviewDocument6 pages00 Biomedical Waste InterviewSp PpvPas encore d'évaluation
- 1 ThesisDocument70 pages1 ThesisSuresh L100% (1)
- F629 15Document3 pagesF629 15masoudPas encore d'évaluation
- EuthanasiaDocument16 pagesEuthanasiaTheresa BreadPas encore d'évaluation
- School of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareDocument13 pagesSchool of Nursing Science and Research (Sharda University) : Assignment ON Alternative Modalities of CareSamjhana Neupane100% (1)
- Histology For RetardsDocument57 pagesHistology For RetardsDavid Degaetano100% (1)
- Trends in Oncology Business DevelopmentDocument25 pagesTrends in Oncology Business DevelopmentSheltie ForeverPas encore d'évaluation
- How To Make Ginger CandyDocument4 pagesHow To Make Ginger CandyJun Jihad BarrogaPas encore d'évaluation
- Apamarga Kshara SwitraDocument6 pagesApamarga Kshara SwitraSamhitha Ayurvedic ChennaiPas encore d'évaluation
- Endometriosis O&g PresentationDocument31 pagesEndometriosis O&g PresentationChauthiran Agamudaiyar100% (1)
- Listeners' Attitudes Toward Children With Voice ProblemsDocument8 pagesListeners' Attitudes Toward Children With Voice ProblemsparismonamourPas encore d'évaluation
- PPK Gigi - DAFTAR ICD 9&ICD 10Document2 pagesPPK Gigi - DAFTAR ICD 9&ICD 10Margarita DewiPas encore d'évaluation
- Estudo Hepasfera Versus BeadDocument6 pagesEstudo Hepasfera Versus BeadAlexandre Campos Moraes AmatoPas encore d'évaluation
- Guidelines For Good Clinical Practice in Clinical Trials (1998)Document49 pagesGuidelines For Good Clinical Practice in Clinical Trials (1998)analyn123Pas encore d'évaluation