Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Basic Science Anaesthesia Update 2008Document200 pagesBasic Science Anaesthesia Update 2008Ruben Kovač100% (1)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- GORUCK Heavy - WEEK 1 PDFDocument1 pageGORUCK Heavy - WEEK 1 PDFJohn RohrerPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Structure and Functions of The EyeDocument16 pagesStructure and Functions of The EyeabdirizakPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Maxillary All-On-Four''Document5 pagesMaxillary All-On-Four''Qiiqa JuarezPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Spinal NervesDocument15 pagesSpinal NervesPrachPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Body Empowerment ThoracisExercisesDocument16 pagesBody Empowerment ThoracisExercisesdracoscribdPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Anatomy of The Respiratory System: Dersi Sayfa Sayfa Türkçe Dinleyin!Document9 pagesAnatomy of The Respiratory System: Dersi Sayfa Sayfa Türkçe Dinleyin!fsdgPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Teaching Advanced Calisthenic MovementsDocument65 pagesTeaching Advanced Calisthenic MovementsAnca Carmen Niculaiasa100% (5)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Body and Face ShapeDocument7 pagesBody and Face ShapeStuti KapoorPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- MAAP Set 2Document86 pagesMAAP Set 2AaronMaroonFive100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- PhysiognomyDocument33 pagesPhysiognomyRalucaFlorentinaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Group Function Occlusion I JosDocument6 pagesGroup Function Occlusion I JosAnonymous gVCIYF6dFPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Skeleton Axial and AppendicularDocument33 pagesSkeleton Axial and AppendicularAnnisa Safira100% (1)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Thyroid ReportDocument3 pagesThyroid ReportArman KhanPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Soal Pra Tentamen KMKDocument3 pagesSoal Pra Tentamen KMKcupacupuPas encore d'évaluation
- Vocal Anatomy: The Journey BeginsDocument16 pagesVocal Anatomy: The Journey Beginstaqadasabbas100% (2)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Arti RehabDocument2 pagesArti RehabTiganaTiganaPas encore d'évaluation
- Soal Unas UGMDocument8 pagesSoal Unas UGMMonik AlamandaPas encore d'évaluation
- Psychology PresentationDocument16 pagesPsychology PresentationFasih RehmanPas encore d'évaluation
- Human Body SIMDocument37 pagesHuman Body SIMRhea Mae S. Sode100% (13)
- 0.2study Guide MSK321. Males. (2022-2023)Document82 pages0.2study Guide MSK321. Males. (2022-2023)truch 2022Pas encore d'évaluation
- Complete Dentures (CDS) - Centric Relation Registration PhasesDocument1 pageComplete Dentures (CDS) - Centric Relation Registration PhasesadiPas encore d'évaluation
- Lesson17 Epithelial CellsDocument22 pagesLesson17 Epithelial CellsGemma WrigleyPas encore d'évaluation
- PDF Make Him Desire You PDF Ebook Alex Carter CompressDocument55 pagesPDF Make Him Desire You PDF Ebook Alex Carter CompresswesavesudanPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- BIMC Update PresentationDocument25 pagesBIMC Update PresentationWahyuPas encore d'évaluation
- Nerve Compression (Entrapment) SyndromeDocument23 pagesNerve Compression (Entrapment) SyndromeTrending razePas encore d'évaluation
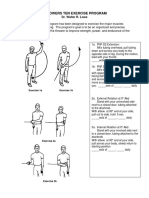
- LP 1throwers - Ten - Exercises - 2010 PDFDocument5 pagesLP 1throwers - Ten - Exercises - 2010 PDFClaudiaPas encore d'évaluation
- Introduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedDocument27 pagesIntroduction To Dental Anatomy: DR - Yad Raouf BDS, Efb, MrcsedRabarPas encore d'évaluation
- Physiology vs. Anatomy: by Sarah C.P. Willaims Medically Reviewed by Minesh Khatri, MD On July 28, 2021Document2 pagesPhysiology vs. Anatomy: by Sarah C.P. Willaims Medically Reviewed by Minesh Khatri, MD On July 28, 2021exo oxePas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- FlatFoot PDFDocument281 pagesFlatFoot PDFJosé Manuel Pena García100% (1)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)