Vous aimerez peut-être aussi
- Research Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionD'EverandResearch Presentations of Dietetic Internship Participants: Research Proceedings - Nutrition and Food SectionPas encore d'évaluation
- Impact of Nutrition Counselling On Multiple Sclerosis Patients Nutritional Status: Randomized Controlled Clinical TrialDocument19 pagesImpact of Nutrition Counselling On Multiple Sclerosis Patients Nutritional Status: Randomized Controlled Clinical Trialmutiara fajriatiPas encore d'évaluation
- Alalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Document4 pagesAlalag, Elsie: "The Impact of Access To Immunization Information On Vaccine Acceptance in Three Countries"Basema HashhashPas encore d'évaluation
- Spirulina ObesidadeDocument10 pagesSpirulina ObesidadeIsabela CastroPas encore d'évaluation
- Relationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewDocument12 pagesRelationship of Knowledge and Attitude With Food Handling Practices: A Systematic ReviewIJPHSPas encore d'évaluation
- Relationship Between Obesity and PeriodontitisDocument4 pagesRelationship Between Obesity and PeriodontitisMadalina MihailaPas encore d'évaluation
- Nutrition StudDocument7 pagesNutrition StudfeelanPas encore d'évaluation
- Shahad 7Document10 pagesShahad 7Mohammed OmarPas encore d'évaluation
- 5 - IJMPS - A Study of Prevalence of Obesity in Adolescents of A Select PrimaryDocument4 pages5 - IJMPS - A Study of Prevalence of Obesity in Adolescents of A Select PrimaryTJPRC PublicationsPas encore d'évaluation
- Inter Gast 4Document11 pagesInter Gast 4tararillalunePas encore d'évaluation
- Study On The Obesity and Nutrition Status of Housewives in Seoul and Kyunggi AreaDocument10 pagesStudy On The Obesity and Nutrition Status of Housewives in Seoul and Kyunggi AreaAwanPas encore d'évaluation
- 4713-7 8.16 Afzaninawati Suria YusofDocument5 pages4713-7 8.16 Afzaninawati Suria Yusof568563Pas encore d'évaluation
- The Association Between UltraDocument10 pagesThe Association Between Ultrasenay.tewolde07Pas encore d'évaluation
- Ijphs Fix B.inggrisDocument14 pagesIjphs Fix B.inggrisrizkimPas encore d'évaluation
- Nutrients 11 03026 v2Document15 pagesNutrients 11 03026 v2ariniPas encore d'évaluation
- A Study On Knowledge and Practice of Mothers of Under-Five ChildrenDocument6 pagesA Study On Knowledge and Practice of Mothers of Under-Five ChildrenRirin PurbaPas encore d'évaluation
- REDALYGDocument8 pagesREDALYGjoel cedeño SánchezPas encore d'évaluation
- Food Sources of Protein and Risk of Incident Gout in The Singapore Chinese Health StudyDocument10 pagesFood Sources of Protein and Risk of Incident Gout in The Singapore Chinese Health StudyoliviaPas encore d'évaluation
- Studying Eating Habits Among Undergraduates College Student at Minia UniversityDocument24 pagesStudying Eating Habits Among Undergraduates College Student at Minia UniversityÁnh NguyễnPas encore d'évaluation
- Impact of Fast Food On Human Health (Vanshita Rajput)Document6 pagesImpact of Fast Food On Human Health (Vanshita Rajput)VANSHITA RAJPUTPas encore d'évaluation
- Integrating Modern Dermatology and AyurvedaDocument25 pagesIntegrating Modern Dermatology and AyurvedachandusgPas encore d'évaluation
- Prevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaDocument6 pagesPrevalence of Self-Medication Practices and Its Associated Factors in Rural Bengaluru, Karnataka, IndiaVijaya RaniPas encore d'évaluation
- ISSN: 0976-3325: TH THDocument3 pagesISSN: 0976-3325: TH THsriwahyuniPas encore d'évaluation
- Ijhrba 03 02 18932Document5 pagesIjhrba 03 02 18932Angie TorresPas encore d'évaluation
- Ewc661 ProposalDocument30 pagesEwc661 ProposalHudal FirdausPas encore d'évaluation
- A Healthy Eating Index To Measure Dietquality in Pregnant Women in Singapore Across-Sectional StudyDocument11 pagesA Healthy Eating Index To Measure Dietquality in Pregnant Women in Singapore Across-Sectional StudyAnisa SafitriPas encore d'évaluation
- Dietary Assessment Methods in Epidemiologic Studies: Epidemiology and HealthDocument8 pagesDietary Assessment Methods in Epidemiologic Studies: Epidemiology and Healthsuhada.akmalPas encore d'évaluation
- 1 s2.0 S2405457723001237 MainDocument7 pages1 s2.0 S2405457723001237 MainAfi FaturPas encore d'évaluation
- JCM 08 00454Document8 pagesJCM 08 00454Harnoor GhumanPas encore d'évaluation
- KonstipasivgfvhDocument16 pagesKonstipasivgfvhrharaPas encore d'évaluation
- Evaluation of The Nutritional Value of Food and Beverages Sold at The Canteen of Far Eastern University - ManilaDocument10 pagesEvaluation of The Nutritional Value of Food and Beverages Sold at The Canteen of Far Eastern University - ManilaPink PastaPas encore d'évaluation
- Fast Food Consumption Pattern and Its Association With Overweight Among High School Boys in Mangalore City of Southern IndiaDocument5 pagesFast Food Consumption Pattern and Its Association With Overweight Among High School Boys in Mangalore City of Southern IndiaAlicia SánchezPas encore d'évaluation
- Prevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersDocument8 pagesPrevalence of Orthorexia Nervosa in University Students and Its Relationship With Psychopathological Aspects of Eating Behaviour DisordersSAMARPITAPas encore d'évaluation
- 7 Skippingmeals PDFDocument10 pages7 Skippingmeals PDFchacaimutPas encore d'évaluation
- 2021 Fad Diets, Body Image, Nutritional Status, and NutritionalDocument5 pages2021 Fad Diets, Body Image, Nutritional Status, and NutritionalLina M GarciaPas encore d'évaluation
- Skrining GiziDocument7 pagesSkrining GiziifaPas encore d'évaluation
- Hajjar Zadeh 2019Document8 pagesHajjar Zadeh 2019TuğbaPas encore d'évaluation
- Prevalence of Malnutrition Among Hospitalized Children: June 2014Document4 pagesPrevalence of Malnutrition Among Hospitalized Children: June 2014Imin BuntaraPas encore d'évaluation
- 5456 26296160 41S PDFDocument6 pages5456 26296160 41S PDFSamaneh TavasoliPas encore d'évaluation
- Medical ScienceDocument6 pagesMedical ScienceRara RabiahPas encore d'évaluation
- Admin,+Journal+Manager,+748 99Z Blinded+Article+File 1451 1-10-20170519Document7 pagesAdmin,+Journal+Manager,+748 99Z Blinded+Article+File 1451 1-10-20170519Putri Hersya MauliaPas encore d'évaluation
- Nutrients 11 00148Document11 pagesNutrients 11 00148Putri N.AprilliaPas encore d'évaluation
- 337.1 s2.0 S0002916522046718 MainDocument10 pages337.1 s2.0 S0002916522046718 MainterePas encore d'évaluation
- A Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.Document5 pagesA Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.International Organization of Scientific Research (IOSR)Pas encore d'évaluation
- The Evaluation and Use of A Food Frequency QuestioDocument14 pagesThe Evaluation and Use of A Food Frequency QuestioprabaPas encore d'évaluation
- A Study On The Relationship Between Mindful Eating, Eating Attitudes and Behaviors and Abdominal Obesity in Adult WomenDocument5 pagesA Study On The Relationship Between Mindful Eating, Eating Attitudes and Behaviors and Abdominal Obesity in Adult WomenInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- The Association Between Eating Habits and Body MasDocument14 pagesThe Association Between Eating Habits and Body MasAngel GonzagaPas encore d'évaluation
- An Investigation On The Effect of Gastric Cancer Education Based On Health Belief Model On Knowledge, Attitude and Nutritional Practice of HousewivesDocument12 pagesAn Investigation On The Effect of Gastric Cancer Education Based On Health Belief Model On Knowledge, Attitude and Nutritional Practice of Housewivesnotrie kristinePas encore d'évaluation
- Ii. Review of Related Literature and StudiesDocument8 pagesIi. Review of Related Literature and Studiesondoy tv100% (1)
- Unhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansDocument7 pagesUnhealthy Food Consumption in Adolescence: Role of Sedentary Behaviours and Modifiers in 11-, 13-And 15-Year-Old ItaliansJason DenostaPas encore d'évaluation
- Hendra Susanto, 2017Document5 pagesHendra Susanto, 2017GREESTYPas encore d'évaluation
- Nutritional and Behavioral Determinants of Adolescent Obesity: A Case - Control Study in Sri LankaDocument6 pagesNutritional and Behavioral Determinants of Adolescent Obesity: A Case - Control Study in Sri LankaStefannyAgnesSalimPas encore d'évaluation
- Poor Dietary Habits: A Function of Online Food Delivery Fad Among Medical and Dental College Students in IndiaDocument8 pagesPoor Dietary Habits: A Function of Online Food Delivery Fad Among Medical and Dental College Students in IndiaA.b.m Nahid Hasan 2115067680Pas encore d'évaluation
- Awareness of Health Consequences of Junk Foods Among Medical StudentsDocument5 pagesAwareness of Health Consequences of Junk Foods Among Medical Studentsprincesspaypa21Pas encore d'évaluation
- PYMS Is A Reliable Malnutrition Screening ToolsDocument8 pagesPYMS Is A Reliable Malnutrition Screening ToolsRika LedyPas encore d'évaluation
- Ijmscr: Knowledge About Supplement and Consumption Behavior Among Grade 10-12 Students in Bangkok, ThailandDocument13 pagesIjmscr: Knowledge About Supplement and Consumption Behavior Among Grade 10-12 Students in Bangkok, ThailandParn (Phitchapa) KittiratanaviwatPas encore d'évaluation
- Health Consciousness and Fast Foods - A Study Among College Students in Lunglei Town, MizoramDocument11 pagesHealth Consciousness and Fast Foods - A Study Among College Students in Lunglei Town, MizoramJoel DarlongPas encore d'évaluation
- Food Suggestions, Meal Frequency and Dietary Diversity Among Pregnant Women A Quantitative StudyDocument12 pagesFood Suggestions, Meal Frequency and Dietary Diversity Among Pregnant Women A Quantitative Studyrian dianaPas encore d'évaluation
- Correlation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaDocument4 pagesCorrelation of Nutritional Anemia and Blood Group Prevalence Among Adolescent Girls in Pudukkottai District of IndiaOmWawanPas encore d'évaluation
- Ba17 PDFDocument16 pagesBa17 PDFScintya NasutionPas encore d'évaluation
- Atm 04 08 160Document9 pagesAtm 04 08 160manalPas encore d'évaluation
- Cold Burn Injuries in The UK: The 11-Year Experience of A Tertiary Burns CentreDocument8 pagesCold Burn Injuries in The UK: The 11-Year Experience of A Tertiary Burns CentremanalPas encore d'évaluation
- Ajr.13.11288 FixDocument12 pagesAjr.13.11288 FixmanalPas encore d'évaluation
- A Novel Technique For The Treatment of Stages III.46 PDFDocument5 pagesA Novel Technique For The Treatment of Stages III.46 PDFmanalPas encore d'évaluation
- Congenital UrogenitalDocument6 pagesCongenital UrogenitalmanalPas encore d'évaluation
- Pengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahDocument7 pagesPengaruh Kenaikan Berat Badan Rata - Rata Per Minggu Pada Kehamilan Trimester Ii Dan Iii Terhadap Risiko Berat Bayi Lahir RendahmanalPas encore d'évaluation
- JCDR 8 DC22 - 2Document4 pagesJCDR 8 DC22 - 2manalPas encore d'évaluation
- Case Report: A Spinal Arteriovenous Fistula in A 3-Year Old BoyDocument5 pagesCase Report: A Spinal Arteriovenous Fistula in A 3-Year Old BoymanalPas encore d'évaluation
- A Detailed Study On Frito LaysDocument12 pagesA Detailed Study On Frito Laysajithjayan199050% (2)
- Vibroshaper Guide: Training & EatingDocument12 pagesVibroshaper Guide: Training & EatingBanica AnisoaraPas encore d'évaluation
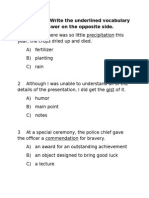
- English E QuizDocument7 pagesEnglish E QuizGrace Amparado UrbanoPas encore d'évaluation
- Booster C Book Molly and The Falcon 1.0Document106 pagesBooster C Book Molly and The Falcon 1.0Mai RamirezPas encore d'évaluation
- Grammar Revision Present Past Future Tenses Questions Modal Verbs PronounsDocument3 pagesGrammar Revision Present Past Future Tenses Questions Modal Verbs PronounsCatarina Pimenta100% (2)
- Tarp Stories Grade Three-1Document14 pagesTarp Stories Grade Three-1GracePas encore d'évaluation
- 2 Substitutes For Non-Vegetarian FoodsDocument30 pages2 Substitutes For Non-Vegetarian FoodsChinju CyrilPas encore d'évaluation
- Grammar Book (Grade 8)Document124 pagesGrammar Book (Grade 8)Vinh NguyenPas encore d'évaluation
- Aussie B2BDocument153 pagesAussie B2BWaf EtanoPas encore d'évaluation
- Buttered Vegetables 1Document1 pageButtered Vegetables 1Christie Mae TorrefielPas encore d'évaluation
- Maggi 2 - Minute NoodleDocument10 pagesMaggi 2 - Minute Noodlealifiya100% (9)
- Cocoa Pest ManagementDocument13 pagesCocoa Pest ManagementAprilia WilonaPas encore d'évaluation
- Brunei DarussalamDocument24 pagesBrunei DarussalamJan Micah MayangPas encore d'évaluation
- Facts About JaejoongDocument25 pagesFacts About JaejoongKumikoPas encore d'évaluation
- Quiz On Hypertension-22March2013Document5 pagesQuiz On Hypertension-22March2013MEPas encore d'évaluation
- Soybean Oil ExtractionDocument22 pagesSoybean Oil ExtractionMuhammad Irfan MalikPas encore d'évaluation
- Basic DialoguesDocument131 pagesBasic DialoguesElizabeth Simão MiguensPas encore d'évaluation
- U2.1 - Simple PresentDocument5 pagesU2.1 - Simple PresentGustavo Nicolás Condor EchevarriaPas encore d'évaluation
- Lebanese Architecture PDFDocument9 pagesLebanese Architecture PDFaboudehPas encore d'évaluation
- Quality Form: Ok Sa Deped - School-Based Feeding Program (SBFP) Program Terminal Report FormDocument8 pagesQuality Form: Ok Sa Deped - School-Based Feeding Program (SBFP) Program Terminal Report FormYunard Yunard100% (2)
- How To Prepare Stock SolutionDocument6 pagesHow To Prepare Stock SolutionaleenaPas encore d'évaluation
- Agus Subarkah - 4611420082 - Assignment TOEFL Structure 4Document3 pagesAgus Subarkah - 4611420082 - Assignment TOEFL Structure 4Agus SubarkahPas encore d'évaluation
- Level 3 Unit 5 ExamDocument3 pagesLevel 3 Unit 5 ExamAlejandra GuarnizoPas encore d'évaluation
- Bangladesh Culture Body ParagraphDocument3 pagesBangladesh Culture Body ParagraphjermPas encore d'évaluation
- SEC 2010 SCIENCE II Integrative Biology TEACHING GUIDE FIRST QUARTER B (CELLULAR STRUCTURES AND FUNCTION)Document14 pagesSEC 2010 SCIENCE II Integrative Biology TEACHING GUIDE FIRST QUARTER B (CELLULAR STRUCTURES AND FUNCTION)DepEdResourcesPas encore d'évaluation
- 2 LP in Creative WritingDocument3 pages2 LP in Creative WritingMeceri Jane Dacuran SilvioPas encore d'évaluation
- PPMC Warehouse Actual Count of Cases (06.23.2023)Document10 pagesPPMC Warehouse Actual Count of Cases (06.23.2023)Alyssa Mae GuroPas encore d'évaluation
- Modo Eng 9Document3 pagesModo Eng 9aaazs2010Pas encore d'évaluation
- 21 Day ConditioningDocument4 pages21 Day ConditioningRoberto A. Ponce de LeonPas encore d'évaluation
- BPP New - PiesDocument24 pagesBPP New - PiesMary Lou ASPas encore d'évaluation