Vous aimerez peut-être aussi
- Angina PectorisDocument36 pagesAngina PectorisBardahWasaLamahPas encore d'évaluation
- IHD. Stable Angina Pectoris Clinical Protocols of The Ministry of Health of THDocument34 pagesIHD. Stable Angina Pectoris Clinical Protocols of The Ministry of Health of THMemories Of j5Pas encore d'évaluation
- Angina (Coronary Artery Disease/Acute Coronary Syndrome) : Care SettingDocument17 pagesAngina (Coronary Artery Disease/Acute Coronary Syndrome) : Care SettingmeghanaPas encore d'évaluation
- Hypertension Concept MapDocument1 pageHypertension Concept Mapgfhbgfhgf71% (7)
- AnginaDocument6 pagesAnginaArslan SaeedPas encore d'évaluation
- PrelimsDocument11 pagesPrelimsJess Fabra100% (1)
- Cardio-Vascular Problems: Group 1Document15 pagesCardio-Vascular Problems: Group 1Reanne Claudine LagunaPas encore d'évaluation
- Angina PectorisDocument30 pagesAngina PectorisTaufik Ramadhan Biya83% (6)
- Atherosclerosis Is The Primary Factor in The Development of CADDocument6 pagesAtherosclerosis Is The Primary Factor in The Development of CADSharlee StonePas encore d'évaluation
- CardiologyDocument9 pagesCardiologyAbi RajasingamPas encore d'évaluation
- Angina PectorisDocument12 pagesAngina Pectorismardsz93% (14)
- Nursing Management Patients W CVD Part2 Myocardial Infarction EnglishDocument43 pagesNursing Management Patients W CVD Part2 Myocardial Infarction EnglishRizka Patria SariPas encore d'évaluation
- Science Time: With Ma'am Melanie!Document28 pagesScience Time: With Ma'am Melanie!Melanie CoronaPas encore d'évaluation
- Angina (Coronary Artery Disease) : Care SettingDocument18 pagesAngina (Coronary Artery Disease) : Care SettingNom NomPas encore d'évaluation
- Presentor: John Hommer E. Dy M.D. Moderator: Joy Marchadesch M.DDocument57 pagesPresentor: John Hommer E. Dy M.D. Moderator: Joy Marchadesch M.DJohn Hommer DyPas encore d'évaluation
- Unstable AnginaDocument5 pagesUnstable AnginaAria AlysisPas encore d'évaluation
- Case Analysis: Medical Surgical NursingDocument7 pagesCase Analysis: Medical Surgical NursingMaria TheresePas encore d'évaluation
- Angina Pectoris: Prepared byDocument30 pagesAngina Pectoris: Prepared byjyothiPas encore d'évaluation
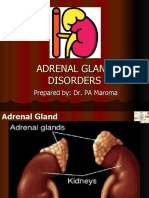
- NCMB 316 Cu14 AdrenalDocument39 pagesNCMB 316 Cu14 AdrenalJanine Dela CruzPas encore d'évaluation
- Angina PectorisDocument12 pagesAngina Pectorisapi-3797941Pas encore d'évaluation
- Angina PectorisDocument8 pagesAngina PectorisPrince DuPas encore d'évaluation
- What Is Angina PectorisDocument2 pagesWhat Is Angina PectorisjesloupayagPas encore d'évaluation
- NCP Angina Coronary Artery DiseaseDocument6 pagesNCP Angina Coronary Artery DiseaseRon Batacan De LeonPas encore d'évaluation
- CV Diet-Fk Modul 4.1 2015Document34 pagesCV Diet-Fk Modul 4.1 2015aryu.kusumastutiPas encore d'évaluation
- NCM Disorders of Myocardial Perfusion-2Document9 pagesNCM Disorders of Myocardial Perfusion-2Jeson Vien GuerraPas encore d'évaluation
- Cardiac Function DisordersDocument8 pagesCardiac Function DisordersAshley MalsonPas encore d'évaluation
- Cardivascular Case Study 4Document57 pagesCardivascular Case Study 4api-302598263Pas encore d'évaluation
- Ischemic Heart Disease, or Coronary Artery Disease: CausesDocument2 pagesIschemic Heart Disease, or Coronary Artery Disease: CausesRandolph AvelinoPas encore d'évaluation
- Stable IHDDocument16 pagesStable IHDDarawan MirzaPas encore d'évaluation
- DR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanDocument50 pagesDR - Datten Bangun MSC - SPFK & DR - Tri Widyawati Msi, PHD Dept - Farmakologi & Therapeutik Fak - Kedokteran Usu MedanHabib Al KahfiPas encore d'évaluation
- Ischemic Heart DiseaseDocument76 pagesIschemic Heart DiseaseNasser AlorfiPas encore d'évaluation
- Drugs For Hypertension 2023Document19 pagesDrugs For Hypertension 2023aguilarjanicaPas encore d'évaluation
- Nclex Study 1Document11 pagesNclex Study 1Katie Shortt100% (4)
- What Symptoms Should Lead The Nurse To Suspect The Pain May Be Angina?Document5 pagesWhat Symptoms Should Lead The Nurse To Suspect The Pain May Be Angina?Dylan Angelo AndresPas encore d'évaluation
- CardioDocument9 pagesCardioVirgilio Reyes ManuelPas encore d'évaluation
- Unstable Angina PectorisDocument28 pagesUnstable Angina PectorisLissaberti AmaliahPas encore d'évaluation
- HypertensionDocument1 pageHypertensionAllyne GavinoPas encore d'évaluation
- Coronary Artery DiseaseDocument15 pagesCoronary Artery DiseaseMuhammad Daha SanusiPas encore d'évaluation
- Cardiovascular SystemDocument205 pagesCardiovascular Systemizuku midoriyaPas encore d'évaluation
- Cardio Ms Hand OutDocument10 pagesCardio Ms Hand OutVictor ShonPas encore d'évaluation
- Asthma:: Case Scenario: DDXDocument10 pagesAsthma:: Case Scenario: DDXFemale calmPas encore d'évaluation
- Chapter 30Document16 pagesChapter 30NurseNancy93Pas encore d'évaluation
- 2myocardial InfarctionDocument29 pages2myocardial Infarctionblessed23Pas encore d'évaluation
- Myocardial InfarctionDocument3 pagesMyocardial Infarctionaja_delPas encore d'évaluation
- Angina PectorisDocument11 pagesAngina Pectorisjialin80% (5)
- Angina Pectoris: Basic InformationDocument3 pagesAngina Pectoris: Basic InformationAsma FerabilPas encore d'évaluation
- ACS (Dr. Thamrin 2015)Document43 pagesACS (Dr. Thamrin 2015)ok sogatenPas encore d'évaluation
- Hypertension (Hypertensive Urgency)Document2 pagesHypertension (Hypertensive Urgency)itsmeayaPas encore d'évaluation
- Pharmacology: Unit VIIIDocument92 pagesPharmacology: Unit VIIIChristian Laraya AlayonPas encore d'évaluation
- Drugs Used To Treat Cardiovascular Diseases: HypertensionDocument35 pagesDrugs Used To Treat Cardiovascular Diseases: HypertensionAyro Business CenterPas encore d'évaluation
- Endocrine Disorders and DrugsDocument149 pagesEndocrine Disorders and DrugsJaypee Fabros Edra100% (1)
- Management & Nursing Care of Patient With Coronary Artery DiseasesDocument49 pagesManagement & Nursing Care of Patient With Coronary Artery DiseaseslouradelPas encore d'évaluation
- Healing Your Heart : The Power of Diet and Homeopathy: Diet, #3D'EverandHealing Your Heart : The Power of Diet and Homeopathy: Diet, #3Pas encore d'évaluation
- Diabetes: Complications of Diabetes: The most important information you need to improve your healthD'EverandDiabetes: Complications of Diabetes: The most important information you need to improve your healthPas encore d'évaluation
- A Simple Guide to Hypertension and Heart DiseasesD'EverandA Simple Guide to Hypertension and Heart DiseasesÉvaluation : 5 sur 5 étoiles5/5 (1)
- How Not To Die From High Blood Pressure - Based On The Teachings Of Michael Greger: Preventing Hypertension And ThrivingD'EverandHow Not To Die From High Blood Pressure - Based On The Teachings Of Michael Greger: Preventing Hypertension And ThrivingPas encore d'évaluation
- Exercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityD'EverandExercise and Diabetes: A Clinician's Guide to Prescribing Physical ActivityPas encore d'évaluation
- CIR-vs-Isabela-Cultural-CorpDocument1 pageCIR-vs-Isabela-Cultural-CorpLizzy WayPas encore d'évaluation
- Duty Free v. COADocument1 pageDuty Free v. COALizzy Way100% (1)
- Winebrenner Inigo Insurance Brokers Inc vs. CIRDocument1 pageWinebrenner Inigo Insurance Brokers Inc vs. CIRLizzy WayPas encore d'évaluation
- MERALCO, Et Al. Vs LimDocument2 pagesMERALCO, Et Al. Vs LimLizzy WayPas encore d'évaluation
- Arches v. BellosilloDocument1 pageArches v. BellosilloLizzy WayPas encore d'évaluation
- Medicard v. CirDocument1 pageMedicard v. CirLizzy WayPas encore d'évaluation
- 2004 Rules On Notarial PracticeDocument14 pages2004 Rules On Notarial PracticeLizzy Way100% (3)
- Electronic Commerce Act (RA No. 8792)Document2 pagesElectronic Commerce Act (RA No. 8792)Lizzy WayPas encore d'évaluation
- Intellectual Property Code (RA No. 8293)Document8 pagesIntellectual Property Code (RA No. 8293)Lizzy WayPas encore d'évaluation
- Basilan Estates vs. CirDocument1 pageBasilan Estates vs. CirLizzy WayPas encore d'évaluation
- Mendez Vs People 726 SCRA 203 (2014)Document1 pageMendez Vs People 726 SCRA 203 (2014)Lizzy WayPas encore d'évaluation
- Sy Po Vs CTADocument1 pageSy Po Vs CTALizzy WayPas encore d'évaluation
- ABAKADA Guro vs. Ermita, 469 SCRA 14Document2 pagesABAKADA Guro vs. Ermita, 469 SCRA 14Lizzy WayPas encore d'évaluation
- Tan Tiong Bio vs. CIR, G.R. No. L-15778, April 23, 1962Document1 pageTan Tiong Bio vs. CIR, G.R. No. L-15778, April 23, 1962Lizzy WayPas encore d'évaluation
- Abakada Guro Party List Vs Ermita GR 168056Document1 pageAbakada Guro Party List Vs Ermita GR 168056Lizzy WayPas encore d'évaluation
- Data Privacy Act (RA No. 10173)Document4 pagesData Privacy Act (RA No. 10173)Lizzy WayPas encore d'évaluation
- PLDT Vs City of BacolodDocument1 pagePLDT Vs City of BacolodLizzy Way100% (1)
- Lutz Vs AranetaDocument1 pageLutz Vs AranetaLizzy WayPas encore d'évaluation
- Lorenzo vs. Posadas Jr.Document2 pagesLorenzo vs. Posadas Jr.Lizzy Way100% (1)
- Paseo Realty and Development CorpDocument1 pagePaseo Realty and Development CorpLizzy WayPas encore d'évaluation
- CIR Vs Eastern TelecommunicationsDocument1 pageCIR Vs Eastern TelecommunicationsLizzy WayPas encore d'évaluation
- Phantom of The OperaDocument18 pagesPhantom of The OperaLizzy Way100% (1)
- CIR V SantosDocument1 pageCIR V SantosLizzy WayPas encore d'évaluation
- Holy Sonnets - Batter My Heart, Three Person'd GodDocument11 pagesHoly Sonnets - Batter My Heart, Three Person'd GodLizzy WayPas encore d'évaluation
- Sarasola v. Trinidad, 40 Phil. 252Document1 pageSarasola v. Trinidad, 40 Phil. 252Lizzy Way100% (1)
- Treatment of EncopresisDocument2 pagesTreatment of Encopresisapi-324904250Pas encore d'évaluation
- Insulin in DMDocument46 pagesInsulin in DMask1400Pas encore d'évaluation
- AIIMS PG Entrance May 2004 Solved Question Paper With KeyDocument15 pagesAIIMS PG Entrance May 2004 Solved Question Paper With KeySAIFPas encore d'évaluation
- Medical para Health-1Document504 pagesMedical para Health-1Yordanos AsmarePas encore d'évaluation
- Interpretation of Mmpi 2 Clinical ScalesDocument23 pagesInterpretation of Mmpi 2 Clinical ScalesJuan LopezPas encore d'évaluation
- Maria Reinares, Eduard Vieta - Integrative Psychotherapy For Bipolar Disorders-Cambridge University Press (2020)Document133 pagesMaria Reinares, Eduard Vieta - Integrative Psychotherapy For Bipolar Disorders-Cambridge University Press (2020)nohanemillerPas encore d'évaluation
- RLE III - A ENT MED Day 2Document6 pagesRLE III - A ENT MED Day 2Kristian Karl Bautista Kiw-isPas encore d'évaluation
- مدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFDocument232 pagesمدونة كل العرب الطبية Davidson - Mcq - 22 - edition PDFنورهانعزالدين100% (1)
- "Focal Infection Theory" States That Bacteria FromDocument2 pages"Focal Infection Theory" States That Bacteria FromBea YmsnPas encore d'évaluation
- COMPLETE Medical Disease in PregnancyDocument210 pagesCOMPLETE Medical Disease in PregnancyCHANDREN ARUMUGAMPas encore d'évaluation
- Haematology-Oncology McqsDocument80 pagesHaematology-Oncology McqsKarim MohamedPas encore d'évaluation
- 4 6048890192880730833Document332 pages4 6048890192880730833Rin4lPas encore d'évaluation
- Experimental Pharmacology: Irrational Drug CombinationsDocument5 pagesExperimental Pharmacology: Irrational Drug CombinationsPrabangkara BillyPas encore d'évaluation
- Dr. Lamia El Wakeel, PhD. Lecturer of Clinical Pharmacy Ain Shams UniversityDocument19 pagesDr. Lamia El Wakeel, PhD. Lecturer of Clinical Pharmacy Ain Shams UniversitysamvetPas encore d'évaluation
- MS Review Exam 5Document10 pagesMS Review Exam 5Gian Karlo GarridoPas encore d'évaluation
- Delos Reyes - Grade 12 - EAPPDocument2 pagesDelos Reyes - Grade 12 - EAPPzavriaPas encore d'évaluation
- OCDDocument51 pagesOCDImon Paul100% (1)
- Guideline Rheumatic Disease in Children PDFDocument432 pagesGuideline Rheumatic Disease in Children PDFMada DobosPas encore d'évaluation
- Visi 71Document196 pagesVisi 71Khoa HữuPas encore d'évaluation
- Prevent Platelet Plugs.: Never IMDocument1 pagePrevent Platelet Plugs.: Never IMdekspeerPas encore d'évaluation
- Accident Reporting ProcedureDocument7 pagesAccident Reporting ProcedureDavid J CRPas encore d'évaluation
- Biology Investigatory Project Xii On Drug AddictionDocument18 pagesBiology Investigatory Project Xii On Drug AddictionKhalifa Shameer60% (5)
- Pakistan Journal of Pharmaceutical Sciences, 23 (4), 449-454 (2010)Document7 pagesPakistan Journal of Pharmaceutical Sciences, 23 (4), 449-454 (2010)Sam SonPas encore d'évaluation
- The Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyDocument9 pagesThe Effects of Cigarette Smoking To The Health of Automotive Grade 11 and Grade 12 Students in Computer Reseacrh Network, INC Background of The StudyRuel OrculloPas encore d'évaluation
- What Is Mental Health or Emotional HealthDocument5 pagesWhat Is Mental Health or Emotional HealthAl LanPas encore d'évaluation
- Momeopathy MM by TAfelDocument321 pagesMomeopathy MM by TAfelKrishan Kumar GargPas encore d'évaluation
- The Wrong Answer: by Harold D. Foster, PHD © 2003Document6 pagesThe Wrong Answer: by Harold D. Foster, PHD © 2003JOSH USHERPas encore d'évaluation
- The Frequency GenerationDocument67 pagesThe Frequency Generationjayjonbeach100% (5)
- Id MMD 2Document9 pagesId MMD 2Nashrah HusnaPas encore d'évaluation
- Basal GangliaDocument40 pagesBasal GangliaEnkefalos KardiaPas encore d'évaluation