Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- 1 - EpidemiologyDocument26 pages1 - Epidemiologyhemihema75% (4)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5795)
- ProstitutionDocument6 pagesProstitutionapi-3763189Pas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Public Health CommentsDocument3 pagesPublic Health CommentsNar Patrick PadillaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Sexually Transmitted InfectionsDocument336 pagesSexually Transmitted Infectionsfalih1959100% (1)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- HookupcultureDocument8 pagesHookupcultureapi-317616298Pas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Lemone/Burke/Bauldoff/Gubrud, Medical-Surgical Nursing 6Th Edition Test BankDocument49 pagesLemone/Burke/Bauldoff/Gubrud, Medical-Surgical Nursing 6Th Edition Test Banknurse homePas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Naguru Provision of Adolescent Friendly Reproductive Health ServicesDocument56 pagesNaguru Provision of Adolescent Friendly Reproductive Health ServicesNdi SimonPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Concept Mapping: Hydatidiform MoleDocument41 pagesConcept Mapping: Hydatidiform MoleDenise FranciscoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sexual SelfDocument18 pagesThe Sexual SelfAngelo Dale Derramas OndilloPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- CCS 010 - HIV, AIDS - Class VER - SEPT 2010 (Autosaved)Document46 pagesCCS 010 - HIV, AIDS - Class VER - SEPT 2010 (Autosaved)Betty SymonPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Related Teenshealth Links: Health Problems SeriesDocument13 pagesRelated Teenshealth Links: Health Problems SeriesMario BadayosPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- I-Science g9 Lesson Plans g9 by D. PhiriDocument49 pagesI-Science g9 Lesson Plans g9 by D. PhiriJoseph NyoniPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Past Locomotor OSCE StationsDocument2 pagesPast Locomotor OSCE Stationsstewart_fPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- NIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewDocument20 pagesNIH Public Access: Provider-Initiated HIV Testing and Counseling in Low-And Middle-Income Countries: A Systematic ReviewAlexandra PaunPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- An Expert System To Provide Sexual and Reproductive Health Educational Contents For Young Deaf WomenDocument5 pagesAn Expert System To Provide Sexual and Reproductive Health Educational Contents For Young Deaf WomenLeonardo JesusPas encore d'évaluation
- Uncle Thors Magazine Summer 2010 (Heathen Asatru Odinist Pagan)Document36 pagesUncle Thors Magazine Summer 2010 (Heathen Asatru Odinist Pagan)Thor SheilPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- TopicDocument5 pagesTopicPrincess OlartePas encore d'évaluation
- MRCP PACES Communication Skills and History Taking NotesDocument44 pagesMRCP PACES Communication Skills and History Taking Notesmehwish sayed100% (1)
- STI Risk & CondomsDocument5 pagesSTI Risk & CondomsAdams LovePas encore d'évaluation
- Unified Work 2021 TeacherDocument11 pagesUnified Work 2021 TeacherJESSIE CUTARAPas encore d'évaluation
- Popdev QuestionsDocument4 pagesPopdev QuestionsMar Angelo TangcangcoPas encore d'évaluation
- MaxMed 2023 SILVER GROUP TOB Category CDocument14 pagesMaxMed 2023 SILVER GROUP TOB Category Cbaashii4Pas encore d'évaluation
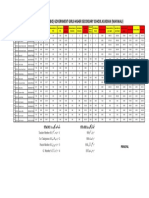
- Merit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Document1 pageMerit List Stis (Bio) Government Girls Higher Secondary School Kundian (Mianwali)Malik AsadPas encore d'évaluation
- Sexually Transmitted InfectionsDocument18 pagesSexually Transmitted InfectionsEthan Matthew Hunt100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- HIV Prevention Programming With Female Sex Workers: A Review of Experiences in Sub-Saharan AfricaDocument21 pagesHIV Prevention Programming With Female Sex Workers: A Review of Experiences in Sub-Saharan Africaapi-26093670Pas encore d'évaluation
- Communicable and Infectious Disease Nursing-NewDocument15 pagesCommunicable and Infectious Disease Nursing-NewShandz de RosasPas encore d'évaluation
- 12月Document149 pages12月Jiandong HanPas encore d'évaluation
- Early Adulthood Development Physical and CogntiiveDocument120 pagesEarly Adulthood Development Physical and CogntiiveKhristian Ross0% (1)
- Socio-Economic Factors Affecting Voluntary Counseling and Testing Services A ReviewDocument37 pagesSocio-Economic Factors Affecting Voluntary Counseling and Testing Services A Reviewlivesource technologyPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Prepregnancy Counseling NoprintDocument11 pagesPrepregnancy Counseling NoprintDo le QuangPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)