Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Punjab Public Service Commission, Lahore: NoticeDocument3 pagesPunjab Public Service Commission, Lahore: NoticeFarhanAwaisiPas encore d'évaluation
- Current Affairs February 1st Week 2021Document27 pagesCurrent Affairs February 1st Week 2021FarhanAwaisiPas encore d'évaluation
- The Time Management Matrix: Manage FocusDocument1 pageThe Time Management Matrix: Manage FocusFarhanAwaisiPas encore d'évaluation
- Tehsil Markaz U.C Segment Name: BarleyDocument55 pagesTehsil Markaz U.C Segment Name: BarleyFarhanAwaisiPas encore d'évaluation
- 1000 MCQs One Paper Book (Everydays Science) by TestPoint - PKDocument65 pages1000 MCQs One Paper Book (Everydays Science) by TestPoint - PKFarhanAwaisi100% (2)
- 650+ Jobs Federal GovtDocument4 pages650+ Jobs Federal GovtFarhanAwaisiPas encore d'évaluation
- Punjab Public Service CommissionDocument2 pagesPunjab Public Service CommissionFarhanAwaisiPas encore d'évaluation
- 22M2019Document12 pages22M2019FarhanAwaisiPas encore d'évaluation
- Most Important Current Affairs MCQs About All Provincial and National AssemblyDocument5 pagesMost Important Current Affairs MCQs About All Provincial and National AssemblyFarhanAwaisiPas encore d'évaluation
- Commission,: Punjab Public ServiceDocument1 pageCommission,: Punjab Public ServiceFarhanAwaisiPas encore d'évaluation
- Award-Winning Culture Guides: UK GuideDocument8 pagesAward-Winning Culture Guides: UK GuideFarhanAwaisiPas encore d'évaluation
- Six Sigma: Sigma's Focus Is On Eliminating Defects and Reducing VariabilityDocument3 pagesSix Sigma: Sigma's Focus Is On Eliminating Defects and Reducing VariabilityFarhanAwaisiPas encore d'évaluation
- PovertyReduction 13 Oct 05Document7 pagesPovertyReduction 13 Oct 05FarhanAwaisiPas encore d'évaluation
- OGDCL Internship Test (Finance and Accounts) Mcqs On 20 August 2017 Batch-2 (White) 1 Biggest Desert (Sahara) 2 Largest River (Nile) 3 Pak Shoertest Boundary With (Chaina)Document1 pageOGDCL Internship Test (Finance and Accounts) Mcqs On 20 August 2017 Batch-2 (White) 1 Biggest Desert (Sahara) 2 Largest River (Nile) 3 Pak Shoertest Boundary With (Chaina)FarhanAwaisiPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Comprehensive Case 2 - QuestionDocument7 pagesComprehensive Case 2 - QuestionPraveen RoshenPas encore d'évaluation
- Deploying MVC5 Based Provider Hosted Apps For On-Premise SharePoint 2013Document22 pagesDeploying MVC5 Based Provider Hosted Apps For On-Premise SharePoint 2013cilango1Pas encore d'évaluation
- Alpine MRV f305Document2 pagesAlpine MRV f305Luis RrPas encore d'évaluation
- Media and Information Literacy Quarter 3 Module 1Document67 pagesMedia and Information Literacy Quarter 3 Module 1Joshua Catequesta100% (1)
- Data Sheet: Permanent Magnet GeneratorDocument2 pagesData Sheet: Permanent Magnet Generatordiegoadjgt100% (1)
- David-Huynh Indeed ResumeDocument3 pagesDavid-Huynh Indeed Resumeapi-546353822Pas encore d'évaluation
- Philippine Multimodal Transportation and Logistics Industry Roadmap - Key Recommendations - 2016.04.14Document89 pagesPhilippine Multimodal Transportation and Logistics Industry Roadmap - Key Recommendations - 2016.04.14PortCalls50% (4)
- Raspberry Pi Installing Noobs OSDocument3 pagesRaspberry Pi Installing Noobs OSEXORCEPas encore d'évaluation
- Taxation Philippine Tax and Income System Assignments and QuizdocxDocument20 pagesTaxation Philippine Tax and Income System Assignments and QuizdocxMicaella ShaynePas encore d'évaluation
- Logbook) Industrial Attachment Brief To Students-3Document6 pagesLogbook) Industrial Attachment Brief To Students-3geybor100% (1)
- BSNL Project MBA NitishDocument92 pagesBSNL Project MBA NitishAnkitSingh0% (2)
- Medicinal Chemistry-Ii: 1.anti-Infective Agents: FDocument14 pagesMedicinal Chemistry-Ii: 1.anti-Infective Agents: FAnonymous ionOPaqlkPas encore d'évaluation
- Compose Testing CheatsheetDocument1 pageCompose Testing CheatsheetEstampados SIn ApellidoPas encore d'évaluation
- Final Exam - Comprehensive - 10.24.16Document5 pagesFinal Exam - Comprehensive - 10.24.16YamatePas encore d'évaluation
- Fouzia AnjumDocument3 pagesFouzia AnjumAbdul SyedPas encore d'évaluation
- Stps 20 H 100 CTDocument8 pagesStps 20 H 100 CTPablo Cruz ArchundiaPas encore d'évaluation
- Heirs of Tancoco v. CADocument28 pagesHeirs of Tancoco v. CAChris YapPas encore d'évaluation
- What Is Bitcoin MiningDocument4 pagesWhat Is Bitcoin MiningCarmen M Leal CurielPas encore d'évaluation
- Kajian Sistematik: Strategi Pembelajaran Klinik Di Setting Rawat JalanDocument5 pagesKajian Sistematik: Strategi Pembelajaran Klinik Di Setting Rawat JalanrhiesnaPas encore d'évaluation
- Soal TKM B. Inggris Kls XII Des. 2013Document8 pagesSoal TKM B. Inggris Kls XII Des. 2013Sinta SilviaPas encore d'évaluation
- Management by ObjectivesDocument30 pagesManagement by ObjectivesJasmandeep brar100% (4)
- CV Rafi Cargill, GAR, MCR, AM GROUP and Consultancy EraDocument6 pagesCV Rafi Cargill, GAR, MCR, AM GROUP and Consultancy EranorulainkPas encore d'évaluation
- SecuritizationDocument46 pagesSecuritizationHitesh MorePas encore d'évaluation
- Part List SR-DVM70AG, SR-DVM70EUDocument28 pagesPart List SR-DVM70AG, SR-DVM70EUAndrea BarbadoroPas encore d'évaluation
- COST v. MMWD Complaint 8.20.19Document64 pagesCOST v. MMWD Complaint 8.20.19Will HoustonPas encore d'évaluation
- Consumer Research ProcessDocument78 pagesConsumer Research ProcessShikha PrasadPas encore d'évaluation
- KINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25Document329 pagesKINDRED HEALTHCARE, INC 10-K (Annual Reports) 2009-02-25http://secwatch.comPas encore d'évaluation
- List of Approved Journals For Promoting Purposes at The University of JordanDocument3 pagesList of Approved Journals For Promoting Purposes at The University of JordanZaid MarwanPas encore d'évaluation
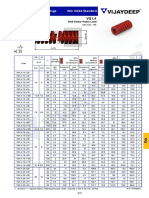
- Rectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadDocument3 pagesRectangular Wire Die Springs ISO-10243 Standard: Red Colour Heavy LoadbashaPas encore d'évaluation
- Variable Length Subnet MasksDocument4 pagesVariable Length Subnet MaskszelalemPas encore d'évaluation