Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Neck Immobilisation TechniqueDocument13 pagesNeck Immobilisation TechniqueAboud AbbassiPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
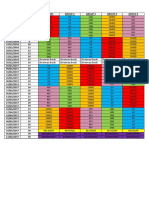
- SC1 Rotations 2016-17Document1 pageSC1 Rotations 2016-17Aboud AbbassiPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Sports Injuries: Class Course Title Lecturer DateDocument41 pagesSports Injuries: Class Course Title Lecturer DatekylieverPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Taking A History of A Patient With A Non TraumaDocument2 pagesTaking A History of A Patient With A Non TraumaAboud AbbassiPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elbow ExaminationelDocument3 pagesElbow ExaminationelAboud AbbassiPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Kablan IbnhaDocument19 pagesKablan IbnhaAboud AbbassiPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Screen Clipping Taken:: Saturday, JulyDocument4 pagesScreen Clipping Taken:: Saturday, JulyAboud AbbassiPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Screen Clipping Taken:: Saturday, JulyDocument4 pagesScreen Clipping Taken:: Saturday, JulyAboud AbbassiPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- 100 Pushups PocketMod (Black and White)Document1 page100 Pushups PocketMod (Black and White)wiredpsychePas encore d'évaluation
- Elbow ExaminationDocument3 pagesElbow ExaminationAboud AbbassiPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- DIT Videos To RewatchDocument2 pagesDIT Videos To RewatchAboud AbbassiPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Nbme 16 AnswersDocument14 pagesNbme 16 AnswersJessica García de Villa71% (14)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- 2015samples Step1Document45 pages2015samples Step1katherinePas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- IC3 Exam Dates 2016 - StudentDocument1 pageIC3 Exam Dates 2016 - StudentAboud AbbassiPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- JC1 Formative Exams 0809 Questions and AnswersDocument8 pagesJC1 Formative Exams 0809 Questions and AnswersAboud AbbassiPas encore d'évaluation
- Primo Surgical Technique - CompressedDocument28 pagesPrimo Surgical Technique - CompressedJuan Martinez Del AngelPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Casts. Braces. TractionDocument3 pagesCasts. Braces. TractionClancy Anne Garcia Naval100% (1)
- Nurseslabs Patient PositioningDocument7 pagesNurseslabs Patient PositioningAilene Ponce FillonPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- X-Ray Patient Positioning Manual 080402Document152 pagesX-Ray Patient Positioning Manual 080402Liev Worth100% (4)
- Case Report OA HipDocument38 pagesCase Report OA HipDian RasitawatiPas encore d'évaluation
- Current Concepts in The Diagnosis and Management of Extraarticular Hip ImpingementDocument8 pagesCurrent Concepts in The Diagnosis and Management of Extraarticular Hip ImpingementClaudio NogueiraPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Kine 3p80 Hip Injury Assignment 2Document4 pagesKine 3p80 Hip Injury Assignment 2api-437399185Pas encore d'évaluation
- Luke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Document3 pagesLuke Vetti - NBPME Part 1 - LEA - Anterior Hip + Gluteal Muscles 1Tyler Lawrence CoyePas encore d'évaluation
- How To Develop The Young QuarterbackDocument47 pagesHow To Develop The Young QuarterbackmunichrangersPas encore d'évaluation
- CT and MR Imaging Ofthe HipDocument11 pagesCT and MR Imaging Ofthe HipsaadPas encore d'évaluation
- The Hip Joint Anatomy: DR Shaifaly Madan RustagiDocument23 pagesThe Hip Joint Anatomy: DR Shaifaly Madan RustagiateoPas encore d'évaluation
- Facilitated Positional Release FPRDocument12 pagesFacilitated Positional Release FPRcoahuiltecoPas encore d'évaluation
- Anatomy VivaDocument5 pagesAnatomy Vivantege stuartPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Dislocation: Muhammad ShahiduzzamanDocument30 pagesDislocation: Muhammad ShahiduzzamanAlicePas encore d'évaluation
- CSC265 Assessment 3Document3 pagesCSC265 Assessment 3software 111Pas encore d'évaluation
- 200 Q& Ans 1Document37 pages200 Q& Ans 1Ghulam DastgeerPas encore d'évaluation
- Workshop Notes: Artist Retreat Zen & The Art of Articulating Dolls by Using BalljointsDocument25 pagesWorkshop Notes: Artist Retreat Zen & The Art of Articulating Dolls by Using BalljointsKristinMytinger91% (11)
- Karate Martial Art and Sport Black Belt Level - Dr. Milorad V. StricevicDocument433 pagesKarate Martial Art and Sport Black Belt Level - Dr. Milorad V. Stricevicbearmiinator67% (3)
- OnBaseU Pitching Manual NotesDocument5 pagesOnBaseU Pitching Manual Noteslw98Pas encore d'évaluation
- Goals of Patient Positioning: Patient Positions in BedDocument4 pagesGoals of Patient Positioning: Patient Positions in Bedjoanna sheenPas encore d'évaluation
- p1310 PDFDocument7 pagesp1310 PDFArya PratamaPas encore d'évaluation
- Low Back Program Exercises - The Nicholas Institute of Sports Medicine and Athletic TraumaDocument7 pagesLow Back Program Exercises - The Nicholas Institute of Sports Medicine and Athletic TraumaRamakrishna KannegantiPas encore d'évaluation
- FIFA The 11+ ManualDocument76 pagesFIFA The 11+ ManualDirk DPas encore d'évaluation
- Anatomy & Physiology - Body Systems: Skeletal System Anatomy QuizDocument5 pagesAnatomy & Physiology - Body Systems: Skeletal System Anatomy QuizmoB0BPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Developmental Dysplasia of The Hip (DDH)Document30 pagesDevelopmental Dysplasia of The Hip (DDH)whidiPas encore d'évaluation
- PRI IntegrationDocument367 pagesPRI IntegrationAnthony Harder100% (7)
- Hip Thrust For Bigger GlutesDocument9 pagesHip Thrust For Bigger GlutesPaul Thomas100% (1)
- Congenital Hip DysplasiaDocument7 pagesCongenital Hip DysplasiaGay PeePas encore d'évaluation
- Pilates For RunnersDocument3 pagesPilates For RunnersCaroline SandryPas encore d'évaluation
- The Yogi Code: Seven Universal Laws of Infinite SuccessD'EverandThe Yogi Code: Seven Universal Laws of Infinite SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (104)