Vous aimerez peut-être aussi
- Table 4. Type of Glaucoma and Association With FailureDocument1 pageTable 4. Type of Glaucoma and Association With FailureJocho NeavesPas encore d'évaluation
- JCM 11 02895Document13 pagesJCM 11 02895Jocho NeavesPas encore d'évaluation
- Day Dreamer: Annette KruisbrinkDocument4 pagesDay Dreamer: Annette KruisbrinkJocho Neaves100% (1)
- Sebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesDocument7 pagesSebaceous Carcinoma of The Eyelids: Personal Experience With 60 CasesJocho NeavesPas encore d'évaluation
- Table 2. Type of Glaucoma and Association With Hypertensive PhaseDocument1 pageTable 2. Type of Glaucoma and Association With Hypertensive PhaseJocho NeavesPas encore d'évaluation
- Dalvin 2017Document28 pagesDalvin 2017Jocho NeavesPas encore d'évaluation
- Choroideremia: Update On Clinical Features and Emerging TreatmentsDocument7 pagesChoroideremia: Update On Clinical Features and Emerging TreatmentsJocho NeavesPas encore d'évaluation
- Cover LetterDocument1 pageCover LetterJocho NeavesPas encore d'évaluation
- Demystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Document14 pagesDemystifying Viral Anterior Uveitis: A Review: Nicole Shu-Wen Chan Mbbs - Soon-Phaik Chee Frcophth Mmed (S'Pore)Dr Pranesh BalasubramaniamPas encore d'évaluation
- Table 1. Demographic and Clinical Characteristics in HP and No HP Groups 0.014Document1 pageTable 1. Demographic and Clinical Characteristics in HP and No HP Groups 0.014Jocho NeavesPas encore d'évaluation
- Erspective: The White Dot SyndromesDocument13 pagesErspective: The White Dot SyndromesJocho NeavesPas encore d'évaluation
- Comparison of 1-Year Outcomes After Ahmed Glaucoma Valve Implantation With and Without Ologen AdjuvantDocument6 pagesComparison of 1-Year Outcomes After Ahmed Glaucoma Valve Implantation With and Without Ologen AdjuvantJocho NeavesPas encore d'évaluation
- Ó 2016 by The American Academy of Ophthalmology Published by Elsevier Inc. ISSN0161-6420/16Document40 pagesÓ 2016 by The American Academy of Ophthalmology Published by Elsevier Inc. ISSN0161-6420/16Jocho NeavesPas encore d'évaluation
- Ocular Features of The HLA-B27-positive Seronegative SpondyloarthropathiesDocument6 pagesOcular Features of The HLA-B27-positive Seronegative SpondyloarthropathiesJocho NeavesPas encore d'évaluation
- Pars Planitis: Epidemiology, Clinical Characteristics, Management and Visual PrognosisDocument12 pagesPars Planitis: Epidemiology, Clinical Characteristics, Management and Visual PrognosisJocho NeavesPas encore d'évaluation
- Ahmed Glaucoma Valve Implant - Surgical Technique and ComplicationsDocument11 pagesAhmed Glaucoma Valve Implant - Surgical Technique and ComplicationsJocho NeavesPas encore d'évaluation
- HHS Public Access: Viral Posterior UveitisDocument62 pagesHHS Public Access: Viral Posterior UveitisJocho NeavesPas encore d'évaluation
- Accepted Manuscript: Survey of OphthalmologyDocument19 pagesAccepted Manuscript: Survey of OphthalmologyJocho NeavesPas encore d'évaluation
- John FerrisDocument485 pagesJohn Ferrissteptaker10Pas encore d'évaluation
- Kjo 32 391Document9 pagesKjo 32 391Jocho NeavesPas encore d'évaluation
- NEUROLOGIADocument2 pagesNEUROLOGIAJocho NeavesPas encore d'évaluation
- Djo 17 013Document8 pagesDjo 17 013Jocho NeavesPas encore d'évaluation
- JCM 09 00416Document12 pagesJCM 09 00416Jocho NeavesPas encore d'évaluation
- Opth 8 1311 PDFDocument6 pagesOpth 8 1311 PDFJocho NeavesPas encore d'évaluation
- Oral Valganciclovir Leads To Higher Exposure To Ganciclovir Than Intravenous Ganciclovir in Patients Following Allogeneic Stem Cell TransplantationDocument8 pagesOral Valganciclovir Leads To Higher Exposure To Ganciclovir Than Intravenous Ganciclovir in Patients Following Allogeneic Stem Cell TransplantationJocho NeavesPas encore d'évaluation
- Wms Main Pocket Guide 2017Document29 pagesWms Main Pocket Guide 2017justrudinPas encore d'évaluation
- Danza Lecumi by Ernesto LecuonaDocument6 pagesDanza Lecumi by Ernesto LecuonaJocho NeavesPas encore d'évaluation
- Sepsis 2015Document10 pagesSepsis 2015Alfred MathewPas encore d'évaluation
- Keratoconus Treatment Algorithm: BackgroundDocument18 pagesKeratoconus Treatment Algorithm: BackgroundJocho NeavesPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Sarina Bakhtiarian 1801853 final exam reviewDocument12 pagesSarina Bakhtiarian 1801853 final exam reviewTop MusicPas encore d'évaluation
- SepsisDocument6 pagesSepsisGigel DumitruPas encore d'évaluation
- SMART-COP Score For Pneumonia Severity - MDCalc 2Document1 pageSMART-COP Score For Pneumonia Severity - MDCalc 2johnlau90Pas encore d'évaluation
- Usb Powered Led Strip: User GuideDocument5 pagesUsb Powered Led Strip: User Guidespiritos123456789Pas encore d'évaluation
- Acute Suppurative Otitis MediaDocument20 pagesAcute Suppurative Otitis MediaNidya PutriPas encore d'évaluation
- The Black DeathDocument6 pagesThe Black DeathjaniPas encore d'évaluation
- WHO Report On Neglected Tropical DiseasesDocument184 pagesWHO Report On Neglected Tropical DiseasesN Aright ForestPas encore d'évaluation
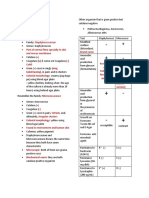
- Mechanism of Action, Spectrum of Activity, Pharmacology, Indications for Use, Toxicity, and Resistance for AntibioticsDocument1 pageMechanism of Action, Spectrum of Activity, Pharmacology, Indications for Use, Toxicity, and Resistance for AntibioticsAduy Hudaya WidihasthaPas encore d'évaluation
- High Yield NBME Images AnnotatedDocument84 pagesHigh Yield NBME Images AnnotatedNareman Abd El HadePas encore d'évaluation
- Psoric BabyDocument5 pagesPsoric BabyAnonymous DPas encore d'évaluation
- UK Biologics Checklist May 2014Document2 pagesUK Biologics Checklist May 2014Dr Sneha's Skin and Allergy Clinic IndiaPas encore d'évaluation
- The Relationship of Population Factors, Water Sources, and Agricultural Areas With The Pandemic of Dengue Hemorrhagic Fever in The COVID-19 Epidemic Situation, Nonthaburi Province, ThailandDocument4 pagesThe Relationship of Population Factors, Water Sources, and Agricultural Areas With The Pandemic of Dengue Hemorrhagic Fever in The COVID-19 Epidemic Situation, Nonthaburi Province, ThailandInternational Journal of Innovative Science and Research TechnologyPas encore d'évaluation
- Antibiotic Resistance Situation in Dhaka BangladeshDocument8 pagesAntibiotic Resistance Situation in Dhaka BangladeshShaheen AkhterPas encore d'évaluation
- PMLS 1 Topic 8.3 TransDocument6 pagesPMLS 1 Topic 8.3 TranslalaPas encore d'évaluation
- Microbial Diseases of The Different Organ System SKINDocument102 pagesMicrobial Diseases of The Different Organ System SKINBea Bianca CruzPas encore d'évaluation
- 2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthDocument11 pages2011 Veterinary Vaccinesand Their Importanceto Animal Healthand Public HealthCARLOTA DIAZ AGUILARPas encore d'évaluation
- Miscellaneous Biochemical TestsDocument45 pagesMiscellaneous Biochemical TestsDale Daniel Macarandan SisonPas encore d'évaluation
- InfluenzaDocument7 pagesInfluenzaGionne Carlo GomezPas encore d'évaluation
- CH nurse epidemic cases community healthDocument12 pagesCH nurse epidemic cases community healthEnrico LavariasPas encore d'évaluation
- REVALIDADocument53 pagesREVALIDAMercy Anne EcatPas encore d'évaluation
- Week 8 - Bacteriology LectureDocument7 pagesWeek 8 - Bacteriology LectureReangg SerranoPas encore d'évaluation
- Blood Donation Frequently Asked QuestionsDocument3 pagesBlood Donation Frequently Asked QuestionsGrace ThairuPas encore d'évaluation
- Cinnamon and HealthDocument14 pagesCinnamon and HealthImani NRPas encore d'évaluation
- National Immunization Program: Manual of Procedures Booklet 7Document32 pagesNational Immunization Program: Manual of Procedures Booklet 7Blue PielagoPas encore d'évaluation
- The Vaccine DebateDocument5 pagesThe Vaccine DebateBeast CheggPas encore d'évaluation
- Started On: Question TextDocument80 pagesStarted On: Question TextSean Lloyd RigonPas encore d'évaluation
- Bba211 Jan20 ExamDocument4 pagesBba211 Jan20 ExamDivine DanielPas encore d'évaluation
- Sec D - Intervention of Common Signs & SymptomsDocument30 pagesSec D - Intervention of Common Signs & SymptomsCheryl OrtizPas encore d'évaluation
- High-risk behaviors and STD prevalence among women prisonersDocument11 pagesHigh-risk behaviors and STD prevalence among women prisonersJOSE LUCEROPas encore d'évaluation
- MM Ous Microscan Clsi Gram Pos Ds 11 2013-01349660Document2 pagesMM Ous Microscan Clsi Gram Pos Ds 11 2013-01349660sazunaxPas encore d'évaluation