Vous aimerez peut-être aussi
- Updated PRC FORM 2015 2016Document6 pagesUpdated PRC FORM 2015 2016Moneto CasaganPas encore d'évaluation
- Mathematical Proof Natural Numbers Well-Ordered Direct ProofDocument5 pagesMathematical Proof Natural Numbers Well-Ordered Direct ProofMoneto CasaganPas encore d'évaluation
- Antiprotozoal DrugsDocument37 pagesAntiprotozoal DrugsMoneto CasaganPas encore d'évaluation
- IntroductionDocument2 pagesIntroductionMoneto CasaganPas encore d'évaluation
- Chapter II LiteratureDocument10 pagesChapter II LiteratureMoneto CasaganPas encore d'évaluation
- Notes: Conceptual Framework For Monitoring and EvaluationDocument8 pagesNotes: Conceptual Framework For Monitoring and EvaluationMoneto CasaganPas encore d'évaluation
- An Introduction To Course And/or Program Evaluation: Mohammad ZohrabiDocument12 pagesAn Introduction To Course And/or Program Evaluation: Mohammad ZohrabiMoneto CasaganPas encore d'évaluation
- ParkinsonsDocument5 pagesParkinsonsMoneto CasaganPas encore d'évaluation
- Pta 41107 3233666 78096Document11 pagesPta 41107 3233666 78096Casey CoxPas encore d'évaluation
- Medical Surgical ManualDocument17 pagesMedical Surgical ManualMoneto CasaganPas encore d'évaluation
- Chapter IIDocument3 pagesChapter IIMoneto CasaganPas encore d'évaluation
- ListDocument1 pageListJennifer JohnstonPas encore d'évaluation
- Attribution of Recent Climate Change Is The Effort To: Further Information:,, andDocument11 pagesAttribution of Recent Climate Change Is The Effort To: Further Information:,, andMoneto CasaganPas encore d'évaluation
- The Normal Newborn Chapt 25, 26, 27Document62 pagesThe Normal Newborn Chapt 25, 26, 27Moneto CasaganPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Lucas MattoonDocument1 pageLucas Mattoonapi-248178524Pas encore d'évaluation
- Portal Hypertension Clinical Features and ManagementDocument29 pagesPortal Hypertension Clinical Features and ManagementPhilip LingPas encore d'évaluation
- Reviewer in Community Health NursingDocument8 pagesReviewer in Community Health NursingFahtma Irene Faye AnayatinPas encore d'évaluation
- Teenage PregnancyDocument12 pagesTeenage PregnancyJoemel Baui85% (13)
- MicroMaxx 3.3 UG ENG P06435-02B e 1 - 1Document200 pagesMicroMaxx 3.3 UG ENG P06435-02B e 1 - 1Waheed MidoPas encore d'évaluation
- Pencak Silat Talent ScoutDocument9 pagesPencak Silat Talent ScoutWisnu Bayu MurtiPas encore d'évaluation
- ATMS Software Tracks Surgical Device TraceabilityDocument27 pagesATMS Software Tracks Surgical Device TraceabilityStenaArapocPas encore d'évaluation
- Understanding the Brain Through Microscopic AnalysisDocument4 pagesUnderstanding the Brain Through Microscopic AnalysisNoah VoelkerPas encore d'évaluation
- 58-Article Text-228-1-10-20180325Document11 pages58-Article Text-228-1-10-20180325mutiara nancyPas encore d'évaluation
- A Harmonious Smile: Biological CostsDocument12 pagesA Harmonious Smile: Biological Costsjsjs kaknsbsPas encore d'évaluation
- Curriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1Document5 pagesCurriculum Map Grade 9 Health: T (N .) M U T C C S P S C S A A R I C V Quarter 1joan niniPas encore d'évaluation
- UK Code of Practice For Tampon Manufactures and DistributorsDocument9 pagesUK Code of Practice For Tampon Manufactures and DistributorsFuzzy_Wood_PersonPas encore d'évaluation
- Lauren Tickner #StrengthFeed Training Guide - 129 PagesDocument129 pagesLauren Tickner #StrengthFeed Training Guide - 129 PagessimplyjimbojimPas encore d'évaluation
- October 2022 Complete Month CA English - CompressedDocument117 pagesOctober 2022 Complete Month CA English - CompressedKing JPas encore d'évaluation
- Karen Horney, Self-Analysis, 1942Document312 pagesKaren Horney, Self-Analysis, 1942Brian EverettPas encore d'évaluation
- FreezingDocument59 pagesFreezingManoj Rathod100% (1)
- The Menace of Immorality Among Nigerian YouthsDocument13 pagesThe Menace of Immorality Among Nigerian Youthsanuoluwapogbenga6Pas encore d'évaluation
- Prevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDDocument7 pagesPrevalence of Pneumonia and Factors Associated Among Children 259 Months Old in Wondo Genet District Sidama Zone SNNPR Ethiopia - PDMusainah FeisalPas encore d'évaluation
- Chirangi vs. StateDocument3 pagesChirangi vs. StateFaithPas encore d'évaluation
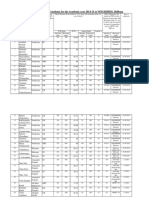
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaPas encore d'évaluation
- Packaged Drinking Water Project ProfileDocument5 pagesPackaged Drinking Water Project ProfileArpna BhatiaPas encore d'évaluation
- Promoting The Rights of Children E3Document15 pagesPromoting The Rights of Children E3api-236865763Pas encore d'évaluation
- Updates On Upper Eyelid Blepharoplasty.4Document8 pagesUpdates On Upper Eyelid Blepharoplasty.4Dimitris RodriguezPas encore d'évaluation
- Practitioner Review of Treatments for AutismDocument18 pagesPractitioner Review of Treatments for AutismAlexandra AddaPas encore d'évaluation
- 4bi1 - Jan22 2b QPDocument28 pages4bi1 - Jan22 2b QPXIN PEIPas encore d'évaluation
- SIWW2024 Water Convention Call For PapersDocument15 pagesSIWW2024 Water Convention Call For PapersAssistant General Manager R&DPas encore d'évaluation
- Soft Drinks in India: Euromonitor International February 2022Document27 pagesSoft Drinks in India: Euromonitor International February 2022Gayathri22394Pas encore d'évaluation
- Acute Tracheobronchitis Causes, Symptoms, TreatmentDocument2 pagesAcute Tracheobronchitis Causes, Symptoms, TreatmentNicole Shannon CariñoPas encore d'évaluation
- MG English Consumer BookletDocument41 pagesMG English Consumer BookletAnh HoaiPas encore d'évaluation
- Wto Unit-2Document19 pagesWto Unit-2Anwar KhanPas encore d'évaluation