Vous aimerez peut-être aussi
- Pharmacology Complete Drug TableDocument6 pagesPharmacology Complete Drug Tableninja-2001100% (4)
- Drug SuffixesDocument3 pagesDrug SuffixesjeromeasuncionPas encore d'évaluation
- Amboss NotesDocument12 pagesAmboss NotesVee Mend100% (2)
- Pharm-Drugs ChartsDocument21 pagesPharm-Drugs ChartsCandace Flowers100% (3)
- Comat NotesDocument33 pagesComat NotesVee Mend100% (1)
- Pharmacology Mnemonics (Part 01) by M IhtishamDocument32 pagesPharmacology Mnemonics (Part 01) by M Ihtishammuhammad ihtisham ul hassan100% (1)
- Sphere: These DiarrheaDocument3 pagesSphere: These Diarrheamed testPas encore d'évaluation
- Antibiotics ChartDocument10 pagesAntibiotics Chartadom09Pas encore d'évaluation
- Top 300 Drugs PDFDocument31 pagesTop 300 Drugs PDFVin Bitz100% (1)
- Antibiotics Study Guide For NursesDocument3 pagesAntibiotics Study Guide For NursesLauren Trotman100% (7)
- CVPR Prototype Drugs TableDocument27 pagesCVPR Prototype Drugs TablethommyvaPas encore d'évaluation
- Pharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsDocument18 pagesPharmacology Drug Chart: Drug Name Receptor Therapeutic Uses Adverse EffectsPadmavathy Naidu Chokkapu100% (2)
- Top 300 DrugsDocument97 pagesTop 300 Drugsstarobin0% (1)
- Pharmacology of HypertensionDocument4 pagesPharmacology of HypertensionFlower100% (1)
- Drug ChartDocument8 pagesDrug Chartstudentalwaysstudy100% (1)
- Micro Buzz Words - KEY WordsDocument8 pagesMicro Buzz Words - KEY WordsKris GulleyPas encore d'évaluation
- Soap TemplateDocument3 pagesSoap TemplaterohitPas encore d'évaluation
- Ninja - Antihyperlipidemics PDFDocument3 pagesNinja - Antihyperlipidemics PDFErica Hyeyeon Lee100% (1)
- Pharmacology Antibiotics - Made Easy DDocument6 pagesPharmacology Antibiotics - Made Easy DHakimah K. Suhaimi0% (1)
- Glomerulonephritis Cheat Sheet PDFDocument1 pageGlomerulonephritis Cheat Sheet PDFAnonymous aA9Ol6239Pas encore d'évaluation
- Comlex EthicsDocument3 pagesComlex EthicsVee MendPas encore d'évaluation
- Antibacterial Drugs SummaryDocument13 pagesAntibacterial Drugs SummaryNeo Ramagaga100% (1)
- Pharmacy MnenomicsDocument12 pagesPharmacy MnenomicsNaresh BabuPas encore d'évaluation
- Acute Complications of Diabetes MellitusDocument1 pageAcute Complications of Diabetes MellitusGerardLum100% (1)
- UWorld Notes Step 2Document93 pagesUWorld Notes Step 2Vee Mend100% (1)
- BED12 - Antibiotics PharmacologyDocument2 pagesBED12 - Antibiotics PharmacologyAmir AmirulPas encore d'évaluation
- Musculoskeletal PharmacologyDocument18 pagesMusculoskeletal PharmacologyBLEEMAGE100% (2)
- Renal Guide and Charts: AlbuminDocument16 pagesRenal Guide and Charts: AlbuminYaima JimenezPas encore d'évaluation
- Drug Interactions 2 Paper PDFDocument2 pagesDrug Interactions 2 Paper PDFAzima AbdelrhamanPas encore d'évaluation
- Pharmacology Chart 3Document2 pagesPharmacology Chart 3Omar ClorPas encore d'évaluation
- Antibiotics Cheat SheetDocument2 pagesAntibiotics Cheat SheetAlejandro Rodas Salinas100% (1)
- Abx FinalDocument3 pagesAbx Finalyanks1120Pas encore d'évaluation
- Pharmacology SummaryDocument16 pagesPharmacology Summaryshenric16Pas encore d'évaluation
- Combank NotesDocument7 pagesCombank NotesVee MendPas encore d'évaluation
- 1617 Biology o Level Top 60 QuestionsDocument39 pages1617 Biology o Level Top 60 QuestionsMeerab ShahPas encore d'évaluation
- Antibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011Document42 pagesAntibiotic Resistance: Audience-Senior Medical Officers Venue-Pune Date - 9 May 2011J NuchinPas encore d'évaluation
- Pharm I - Abx ChartDocument4 pagesPharm I - Abx ChartNicole BerryPas encore d'évaluation
- Total Pharmacy Notes TPN For EEDocument1 601 pagesTotal Pharmacy Notes TPN For EEClaire Cura100% (1)
- Bumetanide Torsemide: Desmopressin - V2Document1 pageBumetanide Torsemide: Desmopressin - V2med testPas encore d'évaluation
- Updated Antibiotic Chart - 2016 PDFDocument2 pagesUpdated Antibiotic Chart - 2016 PDFmugenzi eric100% (1)
- Antibiotics Chart 1Document7 pagesAntibiotics Chart 1Vee MendPas encore d'évaluation
- Drug SummaryDocument5 pagesDrug Summarybriancripe100% (2)
- 2 - What To Use Colloidal Silver For-2016Document24 pages2 - What To Use Colloidal Silver For-2016AB236100% (1)
- A.1. Community-Acquired: Use Antibiotics JudiciouslyDocument33 pagesA.1. Community-Acquired: Use Antibiotics JudiciouslymaxgroovesPas encore d'évaluation
- The Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDocument16 pagesThe Principles of Antibiotic Therapy: S. Aureus Streptococcus PneumoniaeDianne Chua100% (7)
- Review Handouts For Medical Pharmacology: Terriann Crisp, PH.DDocument28 pagesReview Handouts For Medical Pharmacology: Terriann Crisp, PH.Dmus zaharaPas encore d'évaluation
- PCOL Maps PDFDocument11 pagesPCOL Maps PDFZinc YuloPas encore d'évaluation
- Pharmacology: Fast and Dirty Board ReviewDocument7 pagesPharmacology: Fast and Dirty Board ReviewRochelleth7278Pas encore d'évaluation
- Protap KRI Tirta MedikaDocument3 pagesProtap KRI Tirta MedikaZainal Ulu Prima SaputraPas encore d'évaluation
- Pharmacology MapsDocument18 pagesPharmacology MapsPERUBATAN Cawangan Zagazig100% (1)
- Antibiotic Grouping by MechanismDocument11 pagesAntibiotic Grouping by MechanismalterPas encore d'évaluation
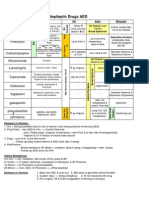
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88Pas encore d'évaluation
- Lile Bai 1: Area/Site Common Organism Useful Abx Other NotesDocument3 pagesLile Bai 1: Area/Site Common Organism Useful Abx Other NotesNicole BerryPas encore d'évaluation
- AntimicrobialsDocument1 pageAntimicrobialsRomaine Barrett100% (1)
- Ninja - Anemias PDFDocument1 pageNinja - Anemias PDFErica Hyeyeon LeePas encore d'évaluation
- Microbiology Step 1 Antimicrobials ChartDocument6 pagesMicrobiology Step 1 Antimicrobials ChartM Patel100% (1)
- Ace Inhibitors MnemonicDocument1 pageAce Inhibitors MnemonicGirish Waru0% (2)
- Internal Medicine #1Document167 pagesInternal Medicine #1Nikhil RayarakulaPas encore d'évaluation
- Complete Drug GuideDocument225 pagesComplete Drug GuideJessica 'Baker' IsaacsPas encore d'évaluation
- GI Diarrheal Micro ChartDocument3 pagesGI Diarrheal Micro ChartEvan MillerPas encore d'évaluation
- AB ClassesDocument4 pagesAB Classesrayooona88100% (2)
- Antibiotic GuideDocument6 pagesAntibiotic GuideAnnTran100% (1)
- Bacterial Flow ChartDocument1 pageBacterial Flow ChartKiana TehraniPas encore d'évaluation
- A. Chemical StructureDocument34 pagesA. Chemical StructureAmit GaurPas encore d'évaluation
- 13 - Antibiotic III Nalidixic AcidDocument7 pages13 - Antibiotic III Nalidixic AcidMoataz TrabehPas encore d'évaluation
- Fixed Dose Combinations: 1. Imipenem + CilastatinDocument8 pagesFixed Dose Combinations: 1. Imipenem + CilastatinNikita SnPas encore d'évaluation
- Chloramphenicol: Ayen University - Al College of PharmacyDocument7 pagesChloramphenicol: Ayen University - Al College of Pharmacyمحمد حميد عطيةPas encore d'évaluation
- Antibacterial SDocument40 pagesAntibacterial SAiman SohailPas encore d'évaluation
- Drug StudyDocument1 pageDrug StudyGeraldine Lopez CostalesPas encore d'évaluation
- Pharma Important Exams TopicsDocument16 pagesPharma Important Exams TopicsMd. Tanvir AhammedPas encore d'évaluation
- Treatment of LeprosyDocument41 pagesTreatment of LeprosyRusty RyanPas encore d'évaluation
- Antibiotic Resistance Situation in Dhaka BangladeshDocument8 pagesAntibiotic Resistance Situation in Dhaka BangladeshShaheen AkhterPas encore d'évaluation
- AttachmentDocument62 pagesAttachmentlevely rizkiPas encore d'évaluation
- Gram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)Document2 pagesGram-Negative Bacteria: Antibiogram of Bacteria - Year 2020 (Icu at Kfafh)jen nalusPas encore d'évaluation
- Highly Effective Against EsblDocument9 pagesHighly Effective Against Esblgaurav rawalPas encore d'évaluation
- Table Handling Obat IntravenaDocument55 pagesTable Handling Obat IntravenaRegita AyuPas encore d'évaluation
- Antimicrobial Activity and Synergistic Effects of Honey and Propolis Produced by Apis Mellifera (European Honeybees)Document32 pagesAntimicrobial Activity and Synergistic Effects of Honey and Propolis Produced by Apis Mellifera (European Honeybees)Euler MendozaPas encore d'évaluation
- OPAT Anti-Infective Administration MethodsDocument6 pagesOPAT Anti-Infective Administration MethodsNikki TranPas encore d'évaluation
- Are Microorganism Boon or Bane? Why?Document2 pagesAre Microorganism Boon or Bane? Why?Ellah GutierrezPas encore d'évaluation
- Usage of Antibiotics in ICU (English)Document13 pagesUsage of Antibiotics in ICU (English)V15CERA FK UNANDPas encore d'évaluation
- Antibiotic Cross-Sensitivity ChartDocument1 pageAntibiotic Cross-Sensitivity ChartChing JuPas encore d'évaluation
- Whonet Documentation: Travancore Medical CollegeDocument20 pagesWhonet Documentation: Travancore Medical Collegetummalapalli venkateswara raoPas encore d'évaluation
- (260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPDocument43 pages(260821) PPT Analsis Evaluasi Penggunaan Obat Di FKTPreginaPas encore d'évaluation
- Laporan Pemakaian Obat Per-PasienDocument2 pagesLaporan Pemakaian Obat Per-Pasienindrawati prasetyaningsihPas encore d'évaluation
- Drug Therapy in Pregnancy (Soal)Document6 pagesDrug Therapy in Pregnancy (Soal)Yola FebriyantiPas encore d'évaluation
- Ashwagandha PharmacokineticsDocument5 pagesAshwagandha PharmacokineticsErshad Shafi AhmedPas encore d'évaluation
- Assignment MicrobioDocument7 pagesAssignment MicrobioHariz BukhariPas encore d'évaluation
- Daftar Dosis ObatDocument3 pagesDaftar Dosis Obatnindy vidyaniPas encore d'évaluation
- A History of The Pharmaceutical IndustryDocument17 pagesA History of The Pharmaceutical IndustryR-A PascualPas encore d'évaluation
- Tugas Analisi 3 JurnalDocument56 pagesTugas Analisi 3 JurnalFatmawati NadhyaPas encore d'évaluation
- Jurnal FarmakokinetikDocument11 pagesJurnal FarmakokinetikNur_Febriana94Pas encore d'évaluation
- Beli ObatDocument54 pagesBeli ObatReynaldi AristaPas encore d'évaluation
- 19 Etest-Price-Guide v8Document2 pages19 Etest-Price-Guide v8Fatima VessaliusPas encore d'évaluation
- Detection of Vancomycin MIC by Agar Dilution in Clinical IsolateDocument11 pagesDetection of Vancomycin MIC by Agar Dilution in Clinical IsolateVamsi KrishnaPas encore d'évaluation
- Co AmoxiclavDocument1 pageCo AmoxiclavMuhammad ArsalanPas encore d'évaluation