Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Ethanol Production From Waste Materials: June 2013Document5 pagesEthanol Production From Waste Materials: June 2013deepu kumarPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- 19 SkyBusDocument5 pages19 SkyBusIfáláwoniléAgboléObemoPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Energy Ethatol Wilson 2009Document48 pagesEnergy Ethatol Wilson 2009IfáláwoniléAgboléObemoPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Ethanol Production From Waste Materials: June 2013Document5 pagesEthanol Production From Waste Materials: June 2013deepu kumarPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Is Iso 21951 2001Document11 pagesIs Iso 21951 2001yesvvnPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Agama Di Kota MalangDocument13 pagesAgama Di Kota MalangIfáláwoniléAgboléObemoPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Amssm Position Statement Concussion in SportDocument13 pagesAmssm Position Statement Concussion in SportIfáláwoniléAgboléObemoPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Alex Barrows Training PDFDocument12 pagesAlex Barrows Training PDFIfáláwoniléAgboléObemo100% (1)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Strategic AlliancesDocument22 pagesStrategic AlliancesAngel Anita100% (2)
- Calculator EngenhariaDocument77 pagesCalculator EngenhariaIfáláwoniléAgboléObemoPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- 2-09 A Graff UsaDocument11 pages2-09 A Graff UsaIfáláwoniléAgboléObemoPas encore d'évaluation
- Vivelle - DOT InglexDocument30 pagesVivelle - DOT InglexIfáláwoniléAgboléObemoPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Supported ID docs for PoI, PoA, PoR, DoBDocument1 pageSupported ID docs for PoI, PoA, PoR, DoBVinit JhingronPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Hurley2001 - Disc AbrasiveDocument7 pagesHurley2001 - Disc AbrasiveIfáláwoniléAgboléObemoPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- Estimated Testing TimesDocument1 pageEstimated Testing TimesIfáláwoniléAgboléObemoPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Mef Country CodesDocument6 pagesMef Country CodesIfáláwoniléAgboléObemoPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Enclothed Cognition ArticleDocument8 pagesEnclothed Cognition ArticlelloydmofPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Shows Mac LarDocument9 pagesShows Mac LarIfáláwoniléAgboléObemoPas encore d'évaluation
- Fast Fact Bullying in SchoolsDocument9 pagesFast Fact Bullying in SchoolsNix DarvishPas encore d'évaluation
- FBI's Evolving Role in Terrorism Investigations Since 9/11Document30 pagesFBI's Evolving Role in Terrorism Investigations Since 9/11IfáláwoniléAgboléObemoPas encore d'évaluation
- Skredderberget - Heaven of Pain - Author's PresentationDocument2 pagesSkredderberget - Heaven of Pain - Author's PresentationIfáláwoniléAgboléObemoPas encore d'évaluation
- CpE194 Lab Experiment # 1 - MTS-88 FamiliarizationDocument4 pagesCpE194 Lab Experiment # 1 - MTS-88 FamiliarizationLouieMurioPas encore d'évaluation
- 7 JitDocument36 pages7 JitFatima AsadPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Tamil Literary Garden 2010 Lifetime Achievement Award CeremonyDocument20 pagesTamil Literary Garden 2010 Lifetime Achievement Award CeremonyAnthony VimalPas encore d'évaluation
- حقيبة تعليمية لمادة التحليلات الهندسية والعدديةDocument28 pagesحقيبة تعليمية لمادة التحليلات الهندسية والعدديةAnjam RasulPas encore d'évaluation
- Liberal Theory: Key Aspects of Idealism in International RelationsDocument11 pagesLiberal Theory: Key Aspects of Idealism in International RelationsArpit JainPas encore d'évaluation
- Finance Process Optimization - Mapping The Journey To High PerformanceDocument3 pagesFinance Process Optimization - Mapping The Journey To High PerformanceStephen G. LynchPas encore d'évaluation
- PLC 2 Ladder DiagramDocument53 pagesPLC 2 Ladder DiagramAnkur GuptaPas encore d'évaluation
- Shailesh Sharma HoroscopeDocument46 pagesShailesh Sharma Horoscopeapi-3818255Pas encore d'évaluation
- Develop Your Kuji In Ability in Body and MindDocument7 pagesDevelop Your Kuji In Ability in Body and MindLenjivac100% (3)
- S32 Design Studio 3.1: NXP SemiconductorsDocument9 pagesS32 Design Studio 3.1: NXP SemiconductorsThành Chu BáPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Math Curriculum Overview Grades 1 8Document1 pageMath Curriculum Overview Grades 1 8GuisellePas encore d'évaluation
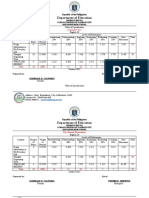
- Table of Specification ENGLISHDocument2 pagesTable of Specification ENGLISHDonn Abel Aguilar IsturisPas encore d'évaluation
- 1 PDFDocument14 pages1 PDFPM JFPas encore d'évaluation
- NIT JRF OpportunityDocument4 pagesNIT JRF Opportunitybalaguru78Pas encore d'évaluation
- Two Monuments by C Mann 1493 Copy - PDF - OcredDocument23 pagesTwo Monuments by C Mann 1493 Copy - PDF - OcredStephania FrancoPas encore d'évaluation
- GR 5 Unit Plan 18-19 Art Warli ArtDocument4 pagesGR 5 Unit Plan 18-19 Art Warli ArtSanjay RautPas encore d'évaluation
- Roadmap For SSC CGLDocument11 pagesRoadmap For SSC CGLibt seoPas encore d'évaluation
- 10 1016@j Ultras 2016 09 002Document11 pages10 1016@j Ultras 2016 09 002Ismahene SmahenoPas encore d'évaluation
- Policarpio 3 - Refresher GEODocument2 pagesPolicarpio 3 - Refresher GEOJohn RoaPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
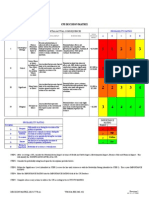
- Decision MatrixDocument12 pagesDecision Matrixrdos14Pas encore d'évaluation
- DPCA OHE Notice of Appeal 4-11-2018 FinalDocument22 pagesDPCA OHE Notice of Appeal 4-11-2018 Finalbranax2000Pas encore d'évaluation
- Instruction Manual For National Security Threat Map UsersDocument16 pagesInstruction Manual For National Security Threat Map UsersJan KastorPas encore d'évaluation
- What Is Science Cornell Notes ExampleDocument3 pagesWhat Is Science Cornell Notes Exampleapi-240096234Pas encore d'évaluation
- Activity Emcee Mid-Year INSET 2021Document3 pagesActivity Emcee Mid-Year INSET 2021Abegail A. Alangue-Calimag67% (6)
- Engineering Mathematics I - Class Test December 2015Document6 pagesEngineering Mathematics I - Class Test December 2015Kunal RamnatsingPas encore d'évaluation
- Indian Oil Corporation- Leading Indian State-Owned Oil and Gas CompanyDocument10 pagesIndian Oil Corporation- Leading Indian State-Owned Oil and Gas CompanyPrakhar ShuklaPas encore d'évaluation
- 5.mpob - LeadershipDocument21 pages5.mpob - LeadershipChaitanya PillalaPas encore d'évaluation
- Humanities Unit Plan Plus Lesson PlansDocument12 pagesHumanities Unit Plan Plus Lesson Plansapi-298200210Pas encore d'évaluation
- Companies DatabaseDocument2 pagesCompanies DatabaseNIRAJ KUMARPas encore d'évaluation
- Bluehill BrochureDocument24 pagesBluehill BrochureGeorge SingerPas encore d'évaluation
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BePas encore d'évaluation
- The Motive: Why So Many Leaders Abdicate Their Most Important ResponsibilitiesD'EverandThe Motive: Why So Many Leaders Abdicate Their Most Important ResponsibilitiesÉvaluation : 5 sur 5 étoiles5/5 (219)
- The 7 Habits of Highly Effective People: The Infographics EditionD'EverandThe 7 Habits of Highly Effective People: The Infographics EditionÉvaluation : 4 sur 5 étoiles4/5 (2475)
- LIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionD'EverandLIT: Life Ignition Tools: Use Nature's Playbook to Energize Your Brain, Spark Ideas, and Ignite ActionÉvaluation : 4 sur 5 étoiles4/5 (402)
- Indistractable: How to Control Your Attention and Choose Your LifeD'EverandIndistractable: How to Control Your Attention and Choose Your LifeÉvaluation : 3.5 sur 5 étoiles3.5/5 (4)