Vous aimerez peut-être aussi
- Unidad Vecinal N°3 - Con AudioDocument8 pagesUnidad Vecinal N°3 - Con Audiobrenda vidarte quispe100% (1)
- Puebla - Es Turismo en PDFDocument32 pagesPuebla - Es Turismo en PDFAndresPimentelAlvarezPas encore d'évaluation
- Catalogo MEXLABDocument51 pagesCatalogo MEXLABAndresPimentelAlvarezPas encore d'évaluation
- NOM-253-SSA1-2012 para La Disposicion de Sangre Humana y Sus Componentes Con Fines TerapeuticosDocument112 pagesNOM-253-SSA1-2012 para La Disposicion de Sangre Humana y Sus Componentes Con Fines TerapeuticosAndresPimentelAlvarezPas encore d'évaluation
- GRR QueratoplastiaPenetranteDocument10 pagesGRR QueratoplastiaPenetranteAndresPimentelAlvarezPas encore d'évaluation
- Blod Bank Hospital Del Sur de MexicoDocument4 pagesBlod Bank Hospital Del Sur de MexicoAndresPimentelAlvarezPas encore d'évaluation
- Gomez Flores Ramos LilianaDocument129 pagesGomez Flores Ramos LilianaAndresPimentelAlvarezPas encore d'évaluation
- Issste 126 08grr PDFDocument6 pagesIssste 126 08grr PDFAndresPimentelAlvarezPas encore d'évaluation
- Edema de Reinke PDFDocument2 pagesEdema de Reinke PDFOscar Alejandro Pongo LalanguiPas encore d'évaluation
- Posicion Es TrasladoDocument3 pagesPosicion Es TrasladoAndresPimentelAlvarezPas encore d'évaluation
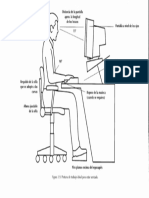
- Postura de Trabajo Ideal para Estar SentadoDocument1 pagePostura de Trabajo Ideal para Estar SentadoAndresPimentelAlvarezPas encore d'évaluation
- Calculos Biliares y Sus ComplicacionesDocument16 pagesCalculos Biliares y Sus ComplicacionesYOshie ParrasPas encore d'évaluation
- Utilidad Del Hidroxietilalmidón Archivos Salud SinaloaDocument5 pagesUtilidad Del Hidroxietilalmidón Archivos Salud SinaloaAndresPimentelAlvarezPas encore d'évaluation
- Trauma TorácicoDocument2 pagesTrauma TorácicoAndresPimentelAlvarezPas encore d'évaluation
- Obsolescencia ProgramadaDocument1 pageObsolescencia ProgramadaAndresPimentelAlvarezPas encore d'évaluation
- OlgivieDocument8 pagesOlgivieAngel X. Luna ZaratePas encore d'évaluation
- Revista Univer CD Juarez 2005Document55 pagesRevista Univer CD Juarez 2005AndresPimentelAlvarezPas encore d'évaluation
- Puebla - Es Turismo en PDFDocument32 pagesPuebla - Es Turismo en PDFAndresPimentelAlvarezPas encore d'évaluation
- Neumonía Adquirida en La Comunidad - Revisión Del Artículo Del NEJM Del 2014Document4 pagesNeumonía Adquirida en La Comunidad - Revisión Del Artículo Del NEJM Del 2014AndresPimentelAlvarezPas encore d'évaluation
- Precios Vento 2017 Vento TiptonicDocument2 pagesPrecios Vento 2017 Vento TiptonicAndresPimentelAlvarezPas encore d'évaluation
- Nutri Info 11 Fresenius KabiDocument20 pagesNutri Info 11 Fresenius KabiAndresPimentelAlvarezPas encore d'évaluation
- Tubo de Torax OJODocument9 pagesTubo de Torax OJOEsau RamirezPas encore d'évaluation
- Precios Vento 2017 Vento Tiptonic PDFDocument2 pagesPrecios Vento 2017 Vento Tiptonic PDFAndresPimentelAlvarezPas encore d'évaluation
- Disfunción Autonómica.Document6 pagesDisfunción Autonómica.arnaldops333Pas encore d'évaluation
- Precios Vento 2017 Vento Tiptonic PDFDocument2 pagesPrecios Vento 2017 Vento Tiptonic PDFAndresPimentelAlvarezPas encore d'évaluation
- Parasitosis en PueblaDocument11 pagesParasitosis en PueblaAndresPimentelAlvarezPas encore d'évaluation
- Hipotiroidismo CongenitoDocument23 pagesHipotiroidismo CongenitoHumberto GüendoPas encore d'évaluation
- Preguntas Farmacologia 2016Document2 pagesPreguntas Farmacologia 2016AndresPimentelAlvarez100% (1)
- 0505 Cancer PulmonDocument10 pages0505 Cancer PulmonAndresPimentelAlvarezPas encore d'évaluation
- Presentación 1Document3 pagesPresentación 1AndresPimentelAlvarezPas encore d'évaluation
- Promo Josue MorochoDocument52 pagesPromo Josue MorochoDevora CabreraPas encore d'évaluation
- Producto PanaderiaDocument87 pagesProducto PanaderiaJohanna Hernandez0% (1)
- Opiniones Legales 2015Document222 pagesOpiniones Legales 2015cinthia mirely tenorio tapia100% (1)
- Acuña Isabel - Sonata de Amor PDFDocument295 pagesAcuña Isabel - Sonata de Amor PDFNoelia Rocío Sanabria100% (2)
- Lineamientos JNSP 2021 Salud Bucal 26 Abril 2021 DEFINITIVODocument16 pagesLineamientos JNSP 2021 Salud Bucal 26 Abril 2021 DEFINITIVORamón Ramírez LópezPas encore d'évaluation
- MAPA MENTAL, Colecistitis Aguda - HFCDocument1 pageMAPA MENTAL, Colecistitis Aguda - HFChugo f.cPas encore d'évaluation
- Ensayo Experimento de Griffith LaliDocument1 pageEnsayo Experimento de Griffith Lalilaura gomezPas encore d'évaluation
- Modelo Reglamento-Interno-De-TrabajoDocument29 pagesModelo Reglamento-Interno-De-Trabajolijica918Pas encore d'évaluation
- UntitledDocument11 pagesUntitledDiana Milena VillamizarPas encore d'évaluation
- Comparacion Iso 45001 y Resolucion 0312Document6 pagesComparacion Iso 45001 y Resolucion 0312Monik BarreraPas encore d'évaluation
- EntradaDocument3 pagesEntradaGabriel SanchezPas encore d'évaluation
- 2388 7212 1 PBDocument7 pages2388 7212 1 PB585mh4krp6Pas encore d'évaluation
- 3 ManipulacionDocument7 pages3 ManipulacionMiller steven Niño tolozaPas encore d'évaluation
- Trabajo de Biologia 1Document5 pagesTrabajo de Biologia 1marvin murgasPas encore d'évaluation
- Oficio Múlt. #204 Remito Bases de Concuros de Buenas Practicas ESIDocument15 pagesOficio Múlt. #204 Remito Bases de Concuros de Buenas Practicas ESINorma TantaPas encore d'évaluation
- r8 Reconocimiento de Las Acciones para El Egreso de La Niña o Niño Del PNCMDocument6 pagesr8 Reconocimiento de Las Acciones para El Egreso de La Niña o Niño Del PNCMDavid Cusihuaman Laura100% (1)
- Microbiologia Ambiental oDocument33 pagesMicrobiologia Ambiental ourl ccPas encore d'évaluation
- Politica de Seguridad y Salud Ocupacional 2013Document1 pagePolitica de Seguridad y Salud Ocupacional 2013Jordy CanalesPas encore d'évaluation
- Protocolo de BioseguridadDocument6 pagesProtocolo de BioseguridadjeffersonPas encore d'évaluation
- Planifico Mi Actividad Fisica - Edwin - DelgadoDocument22 pagesPlanifico Mi Actividad Fisica - Edwin - DelgadoLEANDRO DELGADOPas encore d'évaluation
- Protocolo para La Evaluación de La Severidad Del Abuso Sexual y La Necesidad de Alejar Al Agresor o A La Víctima Del Domicilio FamiliarDocument3 pagesProtocolo para La Evaluación de La Severidad Del Abuso Sexual y La Necesidad de Alejar Al Agresor o A La Víctima Del Domicilio FamiliarNaty ArangoPas encore d'évaluation
- Detección Cualitativa Por PCR de Coronavirus Covid-19 (Sars Cov-2)Document1 pageDetección Cualitativa Por PCR de Coronavirus Covid-19 (Sars Cov-2)Felipe RojasPas encore d'évaluation
- Demencias Una Mirada Biopsicosocial - Budinich - PP 36-40Document6 pagesDemencias Una Mirada Biopsicosocial - Budinich - PP 36-40Gabriel MaxPas encore d'évaluation
- Traumatismo Craneoencefálico.Document2 pagesTraumatismo Craneoencefálico.SAMANTHA DE LILA PRECIADO MARTINEZPas encore d'évaluation
- Estándar de GIRSDocument5 pagesEstándar de GIRSjuanPas encore d'évaluation
- Historia Clinica NeurocirugiaDocument7 pagesHistoria Clinica NeurocirugiaMilagros PichardoPas encore d'évaluation
- SeñalizaciónDocument37 pagesSeñalizaciónJUNIOR TAPIA JIMENEZPas encore d'évaluation
- Charla Se Seguridad RCP BásicaDocument1 pageCharla Se Seguridad RCP BásicaCesar Augusto Gutierrez MendozaPas encore d'évaluation
- Calendario de Equilibrio 2024Document1 pageCalendario de Equilibrio 2024dromanocPas encore d'évaluation