Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Scra 2014Document3 pagesScra 2014Czara DyPas encore d'évaluation
- Marie Ivonne F. Reyes: Pasig Catholic SchoolDocument1 pageMarie Ivonne F. Reyes: Pasig Catholic SchoolCzara DyPas encore d'évaluation
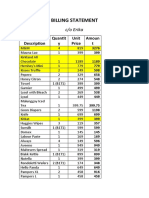
- S&R - Billing StatementDocument4 pagesS&R - Billing StatementCzara DyPas encore d'évaluation
- Banking Mon 7718Document2 pagesBanking Mon 7718Czara DyPas encore d'évaluation
- Castillo vs. RepublicDocument2 pagesCastillo vs. RepublicCzara DyPas encore d'évaluation
- Barcelote Vs - RepublicDocument2 pagesBarcelote Vs - RepublicCzara DyPas encore d'évaluation
- Corpo Notes 2018 PrelimsDocument14 pagesCorpo Notes 2018 PrelimsCzara DyPas encore d'évaluation
- Nil Cases FinalsDocument37 pagesNil Cases FinalsCzara DyPas encore d'évaluation
- G.R. No. L-48955, June 30, 1987)Document8 pagesG.R. No. L-48955, June 30, 1987)Czara DyPas encore d'évaluation
- Institution of Heirs. It Will Not Result To IntestacyDocument9 pagesInstitution of Heirs. It Will Not Result To IntestacyCzara DyPas encore d'évaluation
- Policarpio Vs Active BankDocument2 pagesPolicarpio Vs Active BankCzara DyPas encore d'évaluation
- Sunio v. NLRCDocument3 pagesSunio v. NLRCCzara DyPas encore d'évaluation
- Jimenez vs. FranciscoDocument1 pageJimenez vs. FranciscoCzara DyPas encore d'évaluation
- Q&A Wills Dean AligadaDocument5 pagesQ&A Wills Dean AligadaCzara DyPas encore d'évaluation
- Reynolds v. Ca (Dy)Document2 pagesReynolds v. Ca (Dy)Czara DyPas encore d'évaluation
- Annum From July 1, 2013 Until Full PaymentDocument1 pageAnnum From July 1, 2013 Until Full PaymentCzara DyPas encore d'évaluation
- Memorandum On Charter Change: Presidential Federal ConstitutionDocument1 pageMemorandum On Charter Change: Presidential Federal ConstitutionCzara DyPas encore d'évaluation
- PNB Vs CA DigestDocument3 pagesPNB Vs CA DigestCzara DyPas encore d'évaluation
- Carpio CalaycayDocument4 pagesCarpio CalaycayCzara DyPas encore d'évaluation
- TORTS Page 2 Cases SyllabusDocument77 pagesTORTS Page 2 Cases SyllabusCzara DyPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Concept Map Diagnosis and InterventionsDocument3 pagesConcept Map Diagnosis and Interventionsmenickel3Pas encore d'évaluation
- Cognitive PsychologyDocument10 pagesCognitive Psychologydominscience1Pas encore d'évaluation
- Relationship Between Emotional Intelligence and Psychological Capital With Life Satisfaction in ElderlyDocument8 pagesRelationship Between Emotional Intelligence and Psychological Capital With Life Satisfaction in ElderlyxbachtiarrPas encore d'évaluation
- The Gateway Experience®: Wave V ExploringDocument4 pagesThe Gateway Experience®: Wave V ExploringEvan SchowPas encore d'évaluation
- Importance of Training - Need For Training (2020) - GeektonightDocument7 pagesImportance of Training - Need For Training (2020) - GeektonightMohammed SelimPas encore d'évaluation
- Customer Satisfaction: (Group Members) Salman Hameed Nadir Ali Tariq Khan Asiya Salahuddin Sufyan AhmedDocument36 pagesCustomer Satisfaction: (Group Members) Salman Hameed Nadir Ali Tariq Khan Asiya Salahuddin Sufyan AhmedsalmanPas encore d'évaluation
- Bipolar Disorders - 2023 - Malhi - The Diagnosis of Bipolar Disorder in Children and Adolescents Past Present and FutureDocument9 pagesBipolar Disorders - 2023 - Malhi - The Diagnosis of Bipolar Disorder in Children and Adolescents Past Present and FutureWillams Monte de Souza.Pas encore d'évaluation
- 9 Principles of Learning (Assignment)Document2 pages9 Principles of Learning (Assignment)Arangote Glenn50% (2)
- The Needs Theory: Motivating Employees With Maslow's Hierarchy of Needs - Video & Lesson TranscriptDocument3 pagesThe Needs Theory: Motivating Employees With Maslow's Hierarchy of Needs - Video & Lesson TranscriptOda Red100% (1)
- Background To The Functional Dimensions of Coping (FDC) ScaleDocument5 pagesBackground To The Functional Dimensions of Coping (FDC) Scalejotajota10004950Pas encore d'évaluation
- Values, Attitudes and Job SatisfactionDocument6 pagesValues, Attitudes and Job Satisfaction4gen_7Pas encore d'évaluation
- Week 9 Personal RelationshipDocument5 pagesWeek 9 Personal RelationshipAbdelmar SusulanPas encore d'évaluation
- Etiopathogenesis of DeliriumDocument36 pagesEtiopathogenesis of DeliriumAarti Gupta100% (1)
- Health: Quarter 1 - Module 1 Family HealthDocument18 pagesHealth: Quarter 1 - Module 1 Family HealthCyra100% (1)
- Assessment of Learning 2 Self ReportDocument2 pagesAssessment of Learning 2 Self ReportNicky Burst Uy SeguraPas encore d'évaluation
- Social - Environmental Awareness PostersDocument2 pagesSocial - Environmental Awareness Postersapi-267119096Pas encore d'évaluation
- ModuleDocument4 pagesModuleMerry Joy Tauro Libo-onPas encore d'évaluation
- SSRN Id3121006Document7 pagesSSRN Id3121006Eren Dela CruzPas encore d'évaluation
- (PDF) Download Complete Works of William Shakespeare PDF Ebook by William Shakespeare - Stepor EbookDocument2 pages(PDF) Download Complete Works of William Shakespeare PDF Ebook by William Shakespeare - Stepor EbookAnonymous kJ78MwD4O50% (2)
- Twisting Masculinity: Harms of Pornography To Young Boys and MenDocument8 pagesTwisting Masculinity: Harms of Pornography To Young Boys and MenElvis MtasingwaPas encore d'évaluation
- Grief LossDocument2 pagesGrief Lossapi-491162111Pas encore d'évaluation
- Verbal Warning WorksheetDocument2 pagesVerbal Warning WorksheetAnne ProffittPas encore d'évaluation
- Emotions: DR Aisha Hamdan College of Medicine University of SharjahDocument26 pagesEmotions: DR Aisha Hamdan College of Medicine University of SharjahZainah Ghassan AssafPas encore d'évaluation
- Chapter 7 Communication ApplicationsDocument2 pagesChapter 7 Communication Applicationscarthagecomm28Pas encore d'évaluation
- Home Coach Process Checklist071713Document6 pagesHome Coach Process Checklist071713MyraChPas encore d'évaluation
- HBO NotesDocument4 pagesHBO NotesGrace Ann Soliven EdradaPas encore d'évaluation
- Janina Fisher DISSOCIATIVE PHENOMENA IN THE EVERYDAY LIVES OF TRAUMA SURVIVORSDocument38 pagesJanina Fisher DISSOCIATIVE PHENOMENA IN THE EVERYDAY LIVES OF TRAUMA SURVIVORSMargaret KelomeesPas encore d'évaluation
- Handbook of Emergency Psychiatry 2007Document684 pagesHandbook of Emergency Psychiatry 2007Alicia Carrera Torres100% (3)
- Suggested Classroom Accommodations For Specific BehaviorsDocument9 pagesSuggested Classroom Accommodations For Specific Behaviorsapi-360330020Pas encore d'évaluation
- Neuroscience For CoachesDocument6 pagesNeuroscience For Coachesleejiacheng13636Pas encore d'évaluation