Vous aimerez peut-être aussi
- Pathophysiology CHFDocument3 pagesPathophysiology CHFKit LaraPas encore d'évaluation
- B. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelDocument2 pagesB. Pathophysiology A) Schematic Diagram (Book - Based) : Wasting Blood Glucose LevelCarl Elexer Cuyugan Ano50% (2)
- PATHODocument2 pagesPATHOWendy EscalantePas encore d'évaluation
- Pathogenesis Chronic Complications DiabetesDocument5 pagesPathogenesis Chronic Complications DiabetesGerardLum100% (1)
- Modifiable and Non-Modifiable Risk Factors for Myocardial InfarctionDocument2 pagesModifiable and Non-Modifiable Risk Factors for Myocardial InfarctionWendy Escalante100% (1)
- Angina Pectoris PathophysiologyDocument2 pagesAngina Pectoris Pathophysiologydana86% (7)
- ACS SchematicDocument2 pagesACS Schematicswish27Pas encore d'évaluation
- Optimizing Fluid Therapy in Shock.10Document6 pagesOptimizing Fluid Therapy in Shock.10Paulo Victor100% (1)
- Pathophysiology For HELLP SyndromeDocument2 pagesPathophysiology For HELLP SyndromeRosemarie CarpioPas encore d'évaluation
- Hypertension PathoDocument2 pagesHypertension Pathojake90210100% (1)
- Drugs for Heart FailureDocument39 pagesDrugs for Heart FailureOngKahYeePas encore d'évaluation
- Radicular SyndromeDocument40 pagesRadicular Syndromeainulhawa89Pas encore d'évaluation
- ThrombophiliaDocument3 pagesThrombophiliaGerardLum100% (1)
- Final Myocardial Infarction Pathophysiology PDFDocument3 pagesFinal Myocardial Infarction Pathophysiology PDFDave JoshuaPas encore d'évaluation
- Anemia PathoDocument1 pageAnemia PathoKathleen EvizaPas encore d'évaluation
- Precipitating Factors: Alcoholism Diet ( FAT) Hypertension Predisposing FactorsDocument1 pagePrecipitating Factors: Alcoholism Diet ( FAT) Hypertension Predisposing FactorsKevin Jade HerreraPas encore d'évaluation
- Pathophysiology CVADocument2 pagesPathophysiology CVASewyel Garburi100% (6)
- HTN PathoDocument1 pageHTN PathoShelley Jade MenorPas encore d'évaluation
- Hytension For 16 Years Men (64 Years Old) Cigarette Smoking (32 Pack Years) Alcoholic Drinker For 32 Years Fond of Eating Fatty Foods Physical Inability Sodium Intake HereditaryDocument3 pagesHytension For 16 Years Men (64 Years Old) Cigarette Smoking (32 Pack Years) Alcoholic Drinker For 32 Years Fond of Eating Fatty Foods Physical Inability Sodium Intake HereditaryJohn Paulo CatacutanPas encore d'évaluation
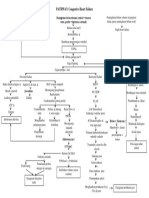
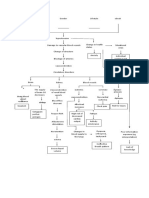
- Pathophysiology Diagram of Congestive Heart FailureDocument3 pagesPathophysiology Diagram of Congestive Heart Failurea_samiane64% (11)
- Pa ToDocument2 pagesPa Tokz392Pas encore d'évaluation
- Case Study - PathophysiologyDocument1 pageCase Study - Pathophysiologychristelleannebabon196Pas encore d'évaluation
- ANGINA PECTORIS Client BasedDocument1 pageANGINA PECTORIS Client BasedGabrielle Gabby Villa RealPas encore d'évaluation
- Pathophysiology HypertensionDocument4 pagesPathophysiology HypertensionKimberly BautistaPas encore d'évaluation
- Hypercholesterolemia Men ( 45 Years Old) Women ( 55 Years Old) Cigarette Smoking Alcoholism Diabetes Mellitus Obesity Physical Inability Sodium Intake HereditaryDocument3 pagesHypercholesterolemia Men ( 45 Years Old) Women ( 55 Years Old) Cigarette Smoking Alcoholism Diabetes Mellitus Obesity Physical Inability Sodium Intake HereditaryMichelle Gliselle Guinto MallarePas encore d'évaluation
- Edema Dan PerdarahanDocument13 pagesEdema Dan PerdarahanKost Vila SakinahPas encore d'évaluation
- Congestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyDocument5 pagesCongestive Heart Failure Secondary To Coronary Artery Disease PathophysiologyJanica MarinasPas encore d'évaluation
- Pathophys BURNDocument2 pagesPathophys BURNpaupaulala83% (6)
- Pa ThoDocument4 pagesPa ThoErnest Genesis Mercado GuevaraPas encore d'évaluation
- Pathophysiology of StrokeDocument3 pagesPathophysiology of StrokeDimple BlancoPas encore d'évaluation
- PATHOPHYSIOLOGYDocument2 pagesPATHOPHYSIOLOGYangeliccat_sweet157992Pas encore d'évaluation
- Lifestyle factors that increase risks of heart disease and pneumoniaDocument1 pageLifestyle factors that increase risks of heart disease and pneumoniaLyssa Marie EgePas encore d'évaluation
- Multisystem ProblemsDocument90 pagesMultisystem ProblemsAlexander Blanche PajelaPas encore d'évaluation
- DM Tipe II Rasa: GDS 203 MG/DL Hba1c 7,3% APTT 22,8 DetikDocument1 pageDM Tipe II Rasa: GDS 203 MG/DL Hba1c 7,3% APTT 22,8 DetikAndrianus AtuPas encore d'évaluation
- Physical Inactivity: Aging Men Hypertension Smoker ObesityDocument1 pagePhysical Inactivity: Aging Men Hypertension Smoker ObesityKEn PilapilPas encore d'évaluation
- Predisposing Factors: Precipitating Factors:: KidneysDocument1 pagePredisposing Factors: Precipitating Factors:: KidneysChe CacatianPas encore d'évaluation
- Myocardial Infarction PathophysiologyDocument3 pagesMyocardial Infarction PathophysiologyPowell TabogocPas encore d'évaluation
- Pa Tho Physiology of Congestive Heart FailureDocument3 pagesPa Tho Physiology of Congestive Heart FailureErin MariePas encore d'évaluation
- Altered Repolarization of The Myocardium: Angina DysrhythmiaDocument3 pagesAltered Repolarization of The Myocardium: Angina DysrhythmiaChen CarpioPas encore d'évaluation
- Pathway Gagal JantungDocument1 pagePathway Gagal Jantungmarlinapsik14Pas encore d'évaluation
- Myocardial Infarction Pathophysiology Schematic DiagramDocument3 pagesMyocardial Infarction Pathophysiology Schematic Diagrammark espirituPas encore d'évaluation
- Myocardial Infarction Pathophysiology Schematic DiagramDocument3 pagesMyocardial Infarction Pathophysiology Schematic Diagrammark espirituPas encore d'évaluation
- Entresto in Insuficienta CardiacaDocument2 pagesEntresto in Insuficienta CardiacaRadu AndreiPas encore d'évaluation
- Antianginal Drugs: Classes Therapeutic Uses MOA Adverse EffectsDocument3 pagesAntianginal Drugs: Classes Therapeutic Uses MOA Adverse EffectsNadhirah ZulkifliPas encore d'évaluation
- Left Sided Heart Failure Dyspnea: Chest PainDocument2 pagesLeft Sided Heart Failure Dyspnea: Chest PainnikinoonaPas encore d'évaluation
- Patoflow Diagram Diabetes Mellitus Baru.1Document2 pagesPatoflow Diagram Diabetes Mellitus Baru.1marlinPas encore d'évaluation
- MIND MAP Walking in PainDocument1 pageMIND MAP Walking in PainDRMAZLINAPas encore d'évaluation
- Heart Rate Blood PressureDocument2 pagesHeart Rate Blood PressureAngelaPas encore d'évaluation
- Pathophysiology of CHF Secondary To RHDDocument89 pagesPathophysiology of CHF Secondary To RHDMira MariantiPas encore d'évaluation
- Darunday NCM 116aDocument3 pagesDarunday NCM 116aEzra Miguel DarundayPas encore d'évaluation
- Pathways to Obesity, Hypertension, and Circulatory DisordersDocument1 pagePathways to Obesity, Hypertension, and Circulatory DisordersFitria NorkhalidaPas encore d'évaluation
- PathwayDocument1 pagePathwayLin DaPas encore d'évaluation
- Renin-Angiotensin-Aldosterone System (Schematic Diagram)Document1 pageRenin-Angiotensin-Aldosterone System (Schematic Diagram)Karl Lourenz DeysolongPas encore d'évaluation
- ST Elevation Myocardial InfarctionDocument1 pageST Elevation Myocardial InfarctionAzizah VillaminPas encore d'évaluation
- Pathway GN PDFDocument2 pagesPathway GN PDFkrniasryPas encore d'évaluation
- Hypertension: Definition and Classification of HypertensionDocument13 pagesHypertension: Definition and Classification of HypertensionnivethitaPas encore d'évaluation
- EMD1 Pc1 PATOFISIOLOGI SEPSISDocument5 pagesEMD1 Pc1 PATOFISIOLOGI SEPSISRasyid RidhaPas encore d'évaluation
- Hemodynamic Disorders Thromboembolic Disease and ShockDocument13 pagesHemodynamic Disorders Thromboembolic Disease and ShockAbu HuraraPas encore d'évaluation
- Anticoagulation TherapyD'EverandAnticoagulation TherapyJoe F. LauPas encore d'évaluation
- Diagnosing Patients With Acute-Onset Persistent DizzinessDocument7 pagesDiagnosing Patients With Acute-Onset Persistent DizzinessMuhammed ElgasimPas encore d'évaluation
- Research PaperDocument32 pagesResearch PaperJillyn FongPas encore d'évaluation
- Anatomy of The KidneysDocument7 pagesAnatomy of The KidneysSanthu SuPas encore d'évaluation
- Hypo Ventilation SyndromesDocument22 pagesHypo Ventilation SyndromesFer45Pas encore d'évaluation
- ValdecoxibDocument3 pagesValdecoxibapi-3797941Pas encore d'évaluation
- Gastritis Erosif PatofisiologiDocument3 pagesGastritis Erosif PatofisiologiLargactil CpzPas encore d'évaluation
- Hepatitis Viruses Combination (Blood Borne Pathogens)Document51 pagesHepatitis Viruses Combination (Blood Borne Pathogens)Hosam GomaaPas encore d'évaluation
- Sample Questions 2Document6 pagesSample Questions 2Filipino Nurses CentralPas encore d'évaluation
- AIHADocument4 pagesAIHAKristine Mae AbrasaldoPas encore d'évaluation
- CPD Jaundice PDFDocument53 pagesCPD Jaundice PDFAnto PaulPas encore d'évaluation
- 1 PE 067 InfographicDocument1 page1 PE 067 InfographicTomáš KrajíčekPas encore d'évaluation
- Aruba TrialDocument8 pagesAruba TrialPatty RiveraPas encore d'évaluation
- ToxoplasmosisDocument22 pagesToxoplasmosisNurrahma FitriyaniPas encore d'évaluation
- Philippine National Police Regional Health Service Ncrpo Physical Examination Guide For Annual Physical Examination (APE)Document2 pagesPhilippine National Police Regional Health Service Ncrpo Physical Examination Guide For Annual Physical Examination (APE)james antonioPas encore d'évaluation
- Checklist Mgu Sabtu 2016Document3 pagesChecklist Mgu Sabtu 2016dudi herlambangPas encore d'évaluation
- Appoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyDocument2 pagesAppoach To Brittle Diabetes: Clinical Algorithm To Determine The EtiologyMudassar SattarPas encore d'évaluation
- Oncology Case StudyDocument3 pagesOncology Case Studyapi-622273373Pas encore d'évaluation
- Whole Blood: Indication of Blood Transfusion With Component Used: Component IndicationsDocument1 pageWhole Blood: Indication of Blood Transfusion With Component Used: Component IndicationsgplabonPas encore d'évaluation
- Small Intestinal Bacterial Overgrowth: A Primary Care ReviewDocument6 pagesSmall Intestinal Bacterial Overgrowth: A Primary Care ReviewjilujPas encore d'évaluation
- Pregabalin: Information For Pain Clinic PatientsDocument6 pagesPregabalin: Information For Pain Clinic PatientsghyonasPas encore d'évaluation
- GROUP 10 Senstive Abt Food and Food AllergiesDocument16 pagesGROUP 10 Senstive Abt Food and Food AllergiesLilis nopita SarryPas encore d'évaluation
- Seborrehic DermatitisDocument25 pagesSeborrehic DermatitisHallidayPas encore d'évaluation
- CC and Mortality ICUDocument8 pagesCC and Mortality ICUSimone BernardesPas encore d'évaluation
- MetabolicsyndDocument37 pagesMetabolicsyndShanooha MansoorPas encore d'évaluation
- Unit 2 - Innovations in Health and Medicine (Paragraphs)Document1 pageUnit 2 - Innovations in Health and Medicine (Paragraphs)April ThunPas encore d'évaluation
- Abdminal Compartment SyndromeDocument9 pagesAbdminal Compartment SyndromeRafael BagusPas encore d'évaluation
- Nama: Sari Wahyuni NPM: 201922074Document4 pagesNama: Sari Wahyuni NPM: 201922074kiki sapriyantiPas encore d'évaluation
- Testimonials Sota 5Document3 pagesTestimonials Sota 5gonzalez1Pas encore d'évaluation