Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Sketchy, Pathoma, BNB ChecklistDocument9 pagesSketchy, Pathoma, BNB ChecklistAC BCPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Aero Medical and First Aid PDFDocument185 pagesAero Medical and First Aid PDFEllene Goglidze100% (2)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Prometric Question BankDocument487 pagesPrometric Question BankLinjumol T GPas encore d'évaluation
- Pre and Post TestsDocument34 pagesPre and Post TestsCher Lenore DesiderioPas encore d'évaluation
- Age Ageing 2003 Petit 19 25Document7 pagesAge Ageing 2003 Petit 19 25BerriFebriantoPas encore d'évaluation
- High Endemicity of Metagonimus Yokogawai Infection Among Residents of Samchok-Shi, Kangwon-DoDocument4 pagesHigh Endemicity of Metagonimus Yokogawai Infection Among Residents of Samchok-Shi, Kangwon-DoBerriFebriantoPas encore d'évaluation
- Epidemiology of Typhoid and Paratyphoid Fever in Kathmandu: Two Years Study and Trends of Antimicrobial ResistanceDocument5 pagesEpidemiology of Typhoid and Paratyphoid Fever in Kathmandu: Two Years Study and Trends of Antimicrobial ResistanceBerriFebriantoPas encore d'évaluation
- Sop For Shimadzu Prominence Hplc1Document1 pageSop For Shimadzu Prominence Hplc1BerriFebriantoPas encore d'évaluation
- Moisturizing LotionDocument19 pagesMoisturizing LotionBerriFebriantoPas encore d'évaluation
- Pharma Midterms Review UwuDocument11 pagesPharma Midterms Review UwuAJ BayPas encore d'évaluation
- 595 July Respiratory Conditions V7Document31 pages595 July Respiratory Conditions V7Ahsan BokhariPas encore d'évaluation
- 2-Shortness of Breath by DR - HananDocument49 pages2-Shortness of Breath by DR - HananSoon SheedPas encore d'évaluation
- Kerala Economy Demographic ProfileDocument52 pagesKerala Economy Demographic ProfileSonia BijuPas encore d'évaluation
- Work-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Document7 pagesWork-Related Chronic Obstructive Pulmonary Disease (COPD) Statistics in Great Britain, 2020Maral GanbilegPas encore d'évaluation
- 8th National Moot CourtDocument12 pages8th National Moot CourtYashasviniPas encore d'évaluation
- Chest ExaminationDocument14 pagesChest Examinationsajad abasewPas encore d'évaluation
- A Case of Pulmonary Aspergilloma and ActinomycosisDocument4 pagesA Case of Pulmonary Aspergilloma and ActinomycosisNova PurbaPas encore d'évaluation
- Key Changes Gold 2023Document15 pagesKey Changes Gold 2023joao cPas encore d'évaluation
- Aerobic Training On Dyspnea Chest Wall CopdDocument8 pagesAerobic Training On Dyspnea Chest Wall CopdBunga Mitra MampuPas encore d'évaluation
- Santi-Total Thesis Title - Upto June 2017Document37 pagesSanti-Total Thesis Title - Upto June 2017SRIKANTA MAJIPas encore d'évaluation
- Gangguan Pernapasan, Kadar Debu Di Pembuatan Batu Bata Di Kecamatan Tenayan RayaDocument7 pagesGangguan Pernapasan, Kadar Debu Di Pembuatan Batu Bata Di Kecamatan Tenayan RayaB2Ayu LestariPas encore d'évaluation
- Determinants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsDocument12 pagesDeterminants of Fitness Level Influencing The Morbidity Rate of Palembang's Hajj PilgrimsSessa MagabePas encore d'évaluation
- ARDS and Resp Failure by SardarDocument53 pagesARDS and Resp Failure by SardarQashqar & GB FolksPas encore d'évaluation
- Medical Surgical Nursing 1st Edition Hoffman Test BankDocument20 pagesMedical Surgical Nursing 1st Edition Hoffman Test Banklilyadelaides4zo100% (29)
- PneumothoraxDocument13 pagesPneumothoraxNooraalnPas encore d'évaluation
- ICD Reference CodesDocument2 pagesICD Reference CodesRavi Pal100% (1)
- Theresa ncp-7Document3 pagesTheresa ncp-7Jovel CortezPas encore d'évaluation
- Copd ImDocument28 pagesCopd ImBianca Watanabe - RatillaPas encore d'évaluation
- Acute Cough: PathophysiologyDocument10 pagesAcute Cough: Pathophysiologysneh1509Pas encore d'évaluation
- MPT CvtsDocument42 pagesMPT CvtsSudarshan100% (1)
- Climate Change and Respiratory InfectionsDocument8 pagesClimate Change and Respiratory InfectionsSara AmorimPas encore d'évaluation
- Care of Patients With Noninfectious Lower Respiratory ProblemsDocument46 pagesCare of Patients With Noninfectious Lower Respiratory Problemsjrflores1284Pas encore d'évaluation
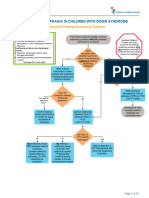
- Aspiration and Dysphagia in Children With Down SyndromeDocument23 pagesAspiration and Dysphagia in Children With Down SyndromeJessa MaePas encore d'évaluation
- Kvir 13 2090071Document12 pagesKvir 13 2090071Familia PipekPas encore d'évaluation