Vous aimerez peut-être aussi
- Nutritional Contribution of Mid-Day Meal (MDM) As Per Quantity Norms at Upper Primary Classes in DelhiDocument17 pagesNutritional Contribution of Mid-Day Meal (MDM) As Per Quantity Norms at Upper Primary Classes in DelhiJASH MATHEWPas encore d'évaluation
- Factors Associated With The Uptake of Cervical Cancer Screening Among Married Women in Udagangoda Grama Niladhari Division, Rathnapura District, Sri LankaDocument4 pagesFactors Associated With The Uptake of Cervical Cancer Screening Among Married Women in Udagangoda Grama Niladhari Division, Rathnapura District, Sri LankaJASH MATHEWPas encore d'évaluation
- Ijsrp p5820 PDFDocument7 pagesIjsrp p5820 PDFJASH MATHEWPas encore d'évaluation
- Factors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiDocument5 pagesFactors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiJASH MATHEWPas encore d'évaluation
- The Role of Information and Communication Technology (ICT) and Early Warning System in School Security Based System in North Eastern NigeriaDocument5 pagesThe Role of Information and Communication Technology (ICT) and Early Warning System in School Security Based System in North Eastern NigeriaJASH MATHEWPas encore d'évaluation
- Biometric Encryption: E-Commerce Security Using Cryptography TechniquesDocument8 pagesBiometric Encryption: E-Commerce Security Using Cryptography TechniquesJASH MATHEWPas encore d'évaluation
- Ijsrp p5819 PDFDocument4 pagesIjsrp p5819 PDFJASH MATHEWPas encore d'évaluation
- Advertisement Analysis: Syntactic Devices in English MagazinesDocument5 pagesAdvertisement Analysis: Syntactic Devices in English MagazinesJASH MATHEWPas encore d'évaluation
- Ijsrp p5818 PDFDocument5 pagesIjsrp p5818 PDFJASH MATHEWPas encore d'évaluation
- Ijsrp p5816 PDFDocument8 pagesIjsrp p5816 PDFJASH MATHEWPas encore d'évaluation
- Factors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiDocument5 pagesFactors Affecting Implementation of Green Procurementin Kenya: A Case Study of Coca-Cola Bottling Limited NairobiJASH MATHEWPas encore d'évaluation
- Synthesis and Characterization of Ɣ-Fe 2 O 3 Nanoparticles Photo Anode by Novel Method For Dye Sensitized Solar CellDocument6 pagesSynthesis and Characterization of Ɣ-Fe 2 O 3 Nanoparticles Photo Anode by Novel Method For Dye Sensitized Solar CellJASH MATHEWPas encore d'évaluation
- Engaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceDocument3 pagesEngaging Students Through Board Games: Measuring Its Effectiveness On Academic PerformanceJASH MATHEWPas encore d'évaluation
- Assessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityDocument5 pagesAssessment of The Use of National Standing Orders in The Treatment of Minor Ailments Among Community Health Practitioners in Ibadan MunicipalityJASH MATHEWPas encore d'évaluation
- F - DERIVATIONS ON BP-ALGEBRASDocument11 pagesF - DERIVATIONS ON BP-ALGEBRASJASH MATHEWPas encore d'évaluation
- The Shift of Focalization in James Joyce's UlyssesDocument7 pagesThe Shift of Focalization in James Joyce's UlyssesJASH MATHEWPas encore d'évaluation
- Linkage Between Water, Sanitation and Health Outcomes:An Empirical Analysis of Indian StatesDocument10 pagesLinkage Between Water, Sanitation and Health Outcomes:An Empirical Analysis of Indian StatesJASH MATHEWPas encore d'évaluation
- Comparative Study of Two Beta - Lactamase Test Methods in Five Different Microorganisms Isolated From Azadi Hospital in Kirkuk, IraqDocument4 pagesComparative Study of Two Beta - Lactamase Test Methods in Five Different Microorganisms Isolated From Azadi Hospital in Kirkuk, IraqJASH MATHEWPas encore d'évaluation
- Analysis of Wage and Labor Productivity in The Hospitality IndustryDocument9 pagesAnalysis of Wage and Labor Productivity in The Hospitality IndustryJASH MATHEWPas encore d'évaluation
- Molecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaDocument7 pagesMolecular Characterization of Extended-Spectrum BetaLactamase (ESBLs) Genes in Pseudomonas Aeruginosa From Pregnant Women Attending A Tertiary Health Care Centre in Makurdi, Central NigeriaJASH MATHEWPas encore d'évaluation
- Combining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaDocument13 pagesCombining Ability Analysis of Early Maturing Maize (Zea Mays.l) Inbred Lines in Central Rift Valley of EthiopiaJASH MATHEWPas encore d'évaluation
- Strategy To Enhance Company's Excellent Performance Case Study: PT Sakalaguna SemestaDocument8 pagesStrategy To Enhance Company's Excellent Performance Case Study: PT Sakalaguna SemestaJASH MATHEWPas encore d'évaluation
- Analysis of Effects of Macroeconomic Variables Against Return On Agriculture StocksDocument8 pagesAnalysis of Effects of Macroeconomic Variables Against Return On Agriculture StocksJASH MATHEWPas encore d'évaluation
- Value Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionDocument5 pagesValue Chain Analysis, at PT. Indofood CBP SuksesMakmurTbk (Noodle DivisionJASH MATHEWPas encore d'évaluation
- Analysis of Poverty Level Fishermen Community Post Tsunami in Aceh, IndonesiaDocument7 pagesAnalysis of Poverty Level Fishermen Community Post Tsunami in Aceh, IndonesiaJASH MATHEWPas encore d'évaluation
- Historical Landscape Quality Assessment On Priority Area of Banda Aceh Heritage City, Aceh ProvinceDocument5 pagesHistorical Landscape Quality Assessment On Priority Area of Banda Aceh Heritage City, Aceh ProvinceJASH MATHEWPas encore d'évaluation
- Effect of Marketing Communications, Brand Equity, Brand Awareness Attitudes and Decision of Customers PT. Mortgage in South SulawesiDocument8 pagesEffect of Marketing Communications, Brand Equity, Brand Awareness Attitudes and Decision of Customers PT. Mortgage in South SulawesiJASH MATHEWPas encore d'évaluation
- Environmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaDocument8 pagesEnvironmental Impact Assessment of Soil Quarrying From The Hills of Central Kerala, Southwest Coast of IndiaJASH MATHEWPas encore d'évaluation
- An Adaptive Study of Symbolic Cultural Items Used at The Nchaka Festival in Ogbaland For Textile Design of IdentityDocument16 pagesAn Adaptive Study of Symbolic Cultural Items Used at The Nchaka Festival in Ogbaland For Textile Design of IdentityJASH MATHEWPas encore d'évaluation
- Hegemonic Masculinity and Oppression of Women in CavedwellerDocument6 pagesHegemonic Masculinity and Oppression of Women in CavedwellerJASH MATHEWPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- MMT Scapular Adduction and Downward Rotation by DR M UsamaDocument25 pagesMMT Scapular Adduction and Downward Rotation by DR M UsamaUsama SohailPas encore d'évaluation
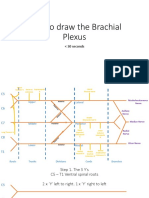
- How To Draw The Brachial PlexusDocument16 pagesHow To Draw The Brachial PlexusHPas encore d'évaluation
- Arnold Schwarzenegger-Bodybuilding EncyclopediaDocument28 pagesArnold Schwarzenegger-Bodybuilding Encyclopediam_armouti100% (4)
- MBs Short PocketsDocument16 pagesMBs Short PocketsIbaiMitxelenaSanchezPas encore d'évaluation
- Handsandfingers PDFDocument3 pagesHandsandfingers PDFiraliral1847Pas encore d'évaluation
- Rig Veda Sandhyavandhanam Telugu PDFDocument16 pagesRig Veda Sandhyavandhanam Telugu PDFSwathi vsPas encore d'évaluation
- Confused AnatomyDocument3 pagesConfused AnatomyAhmed KassemPas encore d'évaluation
- 1.0 Functional Classification of Muscles: Agonist (Prime Mover)Document44 pages1.0 Functional Classification of Muscles: Agonist (Prime Mover)Tan Zhen XinPas encore d'évaluation
- Triada Terrible CCR 09lunes14Document15 pagesTriada Terrible CCR 09lunes14Juan Manuel CastilloPas encore d'évaluation
- Radiological imaging of musculoskeletal and abdominal structuresDocument31 pagesRadiological imaging of musculoskeletal and abdominal structuresNeerupa KissoonPas encore d'évaluation
- Shoulder Anatomy GuideDocument37 pagesShoulder Anatomy GuideevelynPas encore d'évaluation
- Scaphoid Non UnionDocument13 pagesScaphoid Non UnionyahyaPas encore d'évaluation
- Chapter 4 - Wrist BlockDocument6 pagesChapter 4 - Wrist BlockmikayPas encore d'évaluation
- Dissection Notes: Upper Limb MusclesDocument42 pagesDissection Notes: Upper Limb MusclesGeoffreyPas encore d'évaluation
- MCQsDocument9 pagesMCQsratnav_ratanPas encore d'évaluation
- Data Pasien Tindakan DR - JackyDocument42 pagesData Pasien Tindakan DR - JackyStella Putri WandaPas encore d'évaluation
- Anterior Aspect of The Forearm Cubital Fossa 2012Document28 pagesAnterior Aspect of The Forearm Cubital Fossa 2012Elena IftimiPas encore d'évaluation
- KYUSHODocument6 pagesKYUSHOHaya GiriPas encore d'évaluation
- Class 8 - Hand Jue-Yin Pericardium ChannelDocument35 pagesClass 8 - Hand Jue-Yin Pericardium ChannelFrancisco VilaróPas encore d'évaluation
- Hand Surgery Specialty Day 13 Nov 2021: A. Free Papers (7 Min + 3 Min) 10minDocument3 pagesHand Surgery Specialty Day 13 Nov 2021: A. Free Papers (7 Min + 3 Min) 10minFahad HanifPas encore d'évaluation
- Lab 7 Pectoral Girdle 2Document4 pagesLab 7 Pectoral Girdle 2Bechris BambiPas encore d'évaluation
- Railway Accidents and Untoward Incidents (Compensation) Amendment Rules 2016Document5 pagesRailway Accidents and Untoward Incidents (Compensation) Amendment Rules 2016Latest Laws TeamPas encore d'évaluation
- The Hand Complex NEWDocument11 pagesThe Hand Complex NEWVIRESH VPas encore d'évaluation
- Oah Elbow ExercisesDocument4 pagesOah Elbow ExercisesPratik KadamPas encore d'évaluation
- Home Exercise Programs For Musculoskeletal and Sports InjuriesDocument265 pagesHome Exercise Programs For Musculoskeletal and Sports Injuriesvitor flenik100% (5)
- Tennis and Golfer ElbowDocument13 pagesTennis and Golfer Elbowabhay jainPas encore d'évaluation
- Brachial Plexus, DR Adel BondokDocument20 pagesBrachial Plexus, DR Adel BondokSafePas encore d'évaluation
- Cubital Valgus and VarusDocument36 pagesCubital Valgus and VarusHęñøķ BęŕhãñęPas encore d'évaluation
- Green Operative Hand Surgery - Tendon InjuryDocument2 pagesGreen Operative Hand Surgery - Tendon InjurySamuel Jason0% (1)
- Injuries Around The ElbowDocument82 pagesInjuries Around The ElbowNitisha SethiPas encore d'évaluation