Vous aimerez peut-être aussi
- English Vocabulary 2: No. Nama FotoDocument8 pagesEnglish Vocabulary 2: No. Nama Fotofiora.ladesvitaPas encore d'évaluation
- Mahjoob2014 PDFDocument5 pagesMahjoob2014 PDFfiora.ladesvitaPas encore d'évaluation
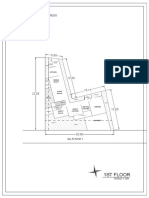
- 1St Floor: House On Paus Schematic Plan ProgressDocument2 pages1St Floor: House On Paus Schematic Plan Progressfiora.ladesvitaPas encore d'évaluation
- Smooth Sailing - Navigating The Sea of Law Applicable To The CruiDocument35 pagesSmooth Sailing - Navigating The Sea of Law Applicable To The Cruifiora.ladesvitaPas encore d'évaluation
- Des An Jose 2019Document6 pagesDes An Jose 2019fiora.ladesvitaPas encore d'évaluation
- Vocab Coco 2Document7 pagesVocab Coco 2fiora.ladesvitaPas encore d'évaluation
- English Vocabulary: No. Nama FotoDocument7 pagesEnglish Vocabulary: No. Nama Fotofiora.ladesvitaPas encore d'évaluation
- Determinants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional StudyDocument10 pagesDeterminants of Delay in Care Seeking Among Children Under Five With Fever in Dodoma Region, Central Tanzania: A Cross-Sectional Studyfiora.ladesvitaPas encore d'évaluation
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaPas encore d'évaluation
- Sex Differences in Cancer Risk and Survival: A Swedish Cohort StudyDocument11 pagesSex Differences in Cancer Risk and Survival: A Swedish Cohort Studyfiora.ladesvitaPas encore d'évaluation
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaPas encore d'évaluation
- Eilers 2007Document12 pagesEilers 2007fiora.ladesvitaPas encore d'évaluation
- F374W1M2L5G52563 FirstDocument1 pageF374W1M2L5G52563 Firstfiora.ladesvitaPas encore d'évaluation
- Childhood Illness Prevalence and Health Seeking Behavior Patterns in Rural TanzaniaDocument12 pagesChildhood Illness Prevalence and Health Seeking Behavior Patterns in Rural Tanzaniafiora.ladesvitaPas encore d'évaluation
- Abdul Kadir 2016Document7 pagesAbdul Kadir 2016fiora.ladesvitaPas encore d'évaluation
- Gibson 2010Document19 pagesGibson 2010fiora.ladesvitaPas encore d'évaluation
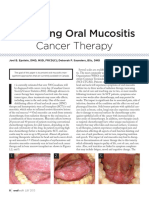
- Managing Oral Mucositis Oral Health July 2015Document4 pagesManaging Oral Mucositis Oral Health July 2015fiora.ladesvitaPas encore d'évaluation
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaPas encore d'évaluation
- Medicalscience: EcancerDocument7 pagesMedicalscience: Ecancerfiora.ladesvitaPas encore d'évaluation
- Abdul Kadir 2016Document7 pagesAbdul Kadir 2016fiora.ladesvitaPas encore d'évaluation
- Quat Trin 2006Document10 pagesQuat Trin 2006fiora.ladesvitaPas encore d'évaluation
- ID Perbandingan Kualitas Hidup Pasien Gagal PDFDocument9 pagesID Perbandingan Kualitas Hidup Pasien Gagal PDFAlawiyahRasyaPas encore d'évaluation
- Full TextDocument127 pagesFull Textfiora.ladesvitaPas encore d'évaluation
- Lalla 2008Document17 pagesLalla 2008fiora.ladesvitaPas encore d'évaluation
- Ambulatory Care Nursing: Coming Soon!Document16 pagesAmbulatory Care Nursing: Coming Soon!fiora.ladesvitaPas encore d'évaluation
- Ni Hms 544150Document15 pagesNi Hms 544150fiora.ladesvitaPas encore d'évaluation
- 2015 Conference 10Document11 pages2015 Conference 10fiora.ladesvitaPas encore d'évaluation
- G15 v03 ED Design Guidelines Dec-14Document77 pagesG15 v03 ED Design Guidelines Dec-14gracegozaliPas encore d'évaluation
- Assessment Rating ScaleDocument8 pagesAssessment Rating Scalefiora.ladesvitaPas encore d'évaluation
- Anderson2004 PDFDocument7 pagesAnderson2004 PDFfiora.ladesvitaPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Adqi Kriteria RifleDocument2 pagesAdqi Kriteria RifleMesa Lina100% (1)
- Pekan 1. Pleno Anatomi KlinisDocument62 pagesPekan 1. Pleno Anatomi KlinisasshyriaPas encore d'évaluation
- Analisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaDocument10 pagesAnalisis Efektivitas Biaya Kombinasi Obat Antihipertensi Pada Pasien Rawat Inap Di Rsud Dr. Soekardjo TasikmalayaEmiPas encore d'évaluation
- 10 Important Blood Tests PART-1 PDFDocument22 pages10 Important Blood Tests PART-1 PDFDimple100% (3)
- Renal ReviewDocument23 pagesRenal ReviewRaven Atisha100% (1)
- Activity 1Document4 pagesActivity 1KyleRepolidon MoralesPas encore d'évaluation
- 7297 19768 4 PBDocument5 pages7297 19768 4 PBpujiindah lestariPas encore d'évaluation
- Curriculum Vitae DR Tan Choon Hian Roger: SpesialisasiDocument2 pagesCurriculum Vitae DR Tan Choon Hian Roger: SpesialisasiRendika BanitrionoPas encore d'évaluation
- How To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPDocument27 pagesHow To Position Finerenone in The Treatment Algorithm For Type 2 Diabetes With Renal Complication - GPMPTaufiqurrokhman RofiiPas encore d'évaluation
- Sca Group 3 Research ProjectDocument23 pagesSca Group 3 Research Projectapi-661170782Pas encore d'évaluation
- Pediatric Malnutrition: Putting The New Definition and Standards Into PracticeDocument16 pagesPediatric Malnutrition: Putting The New Definition and Standards Into PracticeEugenia BocaPas encore d'évaluation
- Medicare Part C Medicare AdvantageDocument3 pagesMedicare Part C Medicare AdvantageJonathan CoutiñoPas encore d'évaluation
- 1610-Article Text-2547-1-10-20220421Document5 pages1610-Article Text-2547-1-10-20220421Fajar JarrPas encore d'évaluation
- Day 13 REDCOPDocument46 pagesDay 13 REDCOPPrabin ChaudharyPas encore d'évaluation
- Nephrology Midt 20 MCQ For StudDocument3 pagesNephrology Midt 20 MCQ For StudMrunal DivePas encore d'évaluation
- Davita ComplaintDocument51 pagesDavita ComplaintbosbydpoPas encore d'évaluation
- Care ManualDocument70 pagesCare ManualQMx2014Pas encore d'évaluation
- Chronic Kidney Disease Stage V: (Laporan Kasus)Document6 pagesChronic Kidney Disease Stage V: (Laporan Kasus)esti wandiraPas encore d'évaluation
- DIET in Chronic Kidney DiseaseDocument3 pagesDIET in Chronic Kidney Diseaseatul_desai_3Pas encore d'évaluation
- Renal 20nutrition 20web 1Document57 pagesRenal 20nutrition 20web 1Qurat ul Ain Arif Sethi Pharmacy PracticePas encore d'évaluation
- Topic Discussion DiabetsDocument30 pagesTopic Discussion Diabetsapi-538856946Pas encore d'évaluation
- D11.44 - Kel10 - Gagal Ginjal KronisDocument16 pagesD11.44 - Kel10 - Gagal Ginjal KronisNAZILLA PUTRIPas encore d'évaluation
- DAFTAR PUSTAKA PU SAYANG Revisi 1Document5 pagesDAFTAR PUSTAKA PU SAYANG Revisi 1REGINAPas encore d'évaluation
- ProteinuriaDocument12 pagesProteinuriaSaraswati Wulandari HartonoPas encore d'évaluation
- Drug Induced Kidney DeseaseDocument12 pagesDrug Induced Kidney DeseaseNurul MasyithahPas encore d'évaluation
- Jurnal Gangguan GinjalDocument11 pagesJurnal Gangguan GinjalCut IklimaPas encore d'évaluation
- Acute Kidney InjuryDocument49 pagesAcute Kidney InjuryfikasywPas encore d'évaluation
- Appendix C: Tables, Conversions and AbbreviationsDocument2 pagesAppendix C: Tables, Conversions and AbbreviationsBrian FoongPas encore d'évaluation
- Chronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaDocument62 pagesChronic Kidney Disease: Presented By, Mariya Antony 3 Year BSC Nursing ST - Thomas College of Nursing ChethipuzhaSamuel LalPas encore d'évaluation
- Quality of Life in Patients With End Stage Renal Disease On HemodialysisDocument11 pagesQuality of Life in Patients With End Stage Renal Disease On HemodialysisAmalia UtamiPas encore d'évaluation