Vous aimerez peut-être aussi
- BBasic ECG Part1-1Document58 pagesBBasic ECG Part1-1Annsha VeimernPas encore d'évaluation
- CefixmeDocument1 pageCefixmeAnnsha VeimernPas encore d'évaluation
- Common Icu Drips PDFDocument1 pageCommon Icu Drips PDFAnnsha VeimernPas encore d'évaluation
- Color Atlas of MalariaDocument2 pagesColor Atlas of MalariaOrangeetPas encore d'évaluation
- WHO RHR 15.07 Eng PDFDocument14 pagesWHO RHR 15.07 Eng PDFAnnsha VeimernPas encore d'évaluation
- A B C D E: Advanced Trauma Life Support - AtlsDocument2 pagesA B C D E: Advanced Trauma Life Support - AtlsAnnsha VeimernPas encore d'évaluation
- Physeal AnatomyDocument5 pagesPhyseal AnatomyAnnsha VeimernPas encore d'évaluation
- Malaria Microscopy: Quality Assurance ManualDocument140 pagesMalaria Microscopy: Quality Assurance ManualAnnsha VeimernPas encore d'évaluation
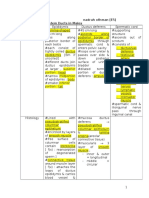
- Reproductive System Ducts in MalesDocument10 pagesReproductive System Ducts in MalesAnnsha VeimernPas encore d'évaluation
- Case 2Document4 pagesCase 2Annsha VeimernPas encore d'évaluation
- FungalDocument3 pagesFungalAnnsha VeimernPas encore d'évaluation
- Plasmodium Ovale: Laboratory Diagnosis of MalariaDocument4 pagesPlasmodium Ovale: Laboratory Diagnosis of MalariaFitrah QolbinaPas encore d'évaluation
- DrugDocument4 pagesDrugAnnsha VeimernPas encore d'évaluation
- ToxoplasmosisDocument6 pagesToxoplasmosisAnnsha Veimern100% (1)
- Management of Blood TransfusionDocument2 pagesManagement of Blood TransfusionAnnsha VeimernPas encore d'évaluation
- Gram Stain BacteriaDocument6 pagesGram Stain BacteriaAnnsha VeimernPas encore d'évaluation
- Clinical ManifestationsDocument4 pagesClinical ManifestationsAnnsha VeimernPas encore d'évaluation
- MenstruationDocument16 pagesMenstruationAnnsha VeimernPas encore d'évaluation
- Gram Stain BacteriaDocument6 pagesGram Stain BacteriaAnnsha VeimernPas encore d'évaluation
- Mention The Origin of The Culture!Document4 pagesMention The Origin of The Culture!Annsha VeimernPas encore d'évaluation
- Neonatal Sepsis Types Early Late OnsetDocument1 pageNeonatal Sepsis Types Early Late OnsetAnnsha VeimernPas encore d'évaluation
- MalnutritionDocument8 pagesMalnutritionAnnsha VeimernPas encore d'évaluation
- Lactose IntolerencDocument4 pagesLactose IntolerencAnnsha VeimernPas encore d'évaluation
- Gram Stain BacteriaDocument6 pagesGram Stain BacteriaAnnsha VeimernPas encore d'évaluation
- Prognosis Apprisal Sheet PDFDocument2 pagesPrognosis Apprisal Sheet PDFAkhmad AfriantoPas encore d'évaluation
- Experiment BioDocument3 pagesExperiment BioAnnsha VeimernPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Fat Burn ConceptDocument31 pagesFat Burn ConceptManoj100% (1)
- Bac ToxinDocument9 pagesBac ToxinJawairia KhawarPas encore d'évaluation
- Arab Board Orthopedic Exam June 2013Document35 pagesArab Board Orthopedic Exam June 2013Nasser AlbaddaiPas encore d'évaluation
- 12 White Blood Cell Counting Techniques in BirdsDocument5 pages12 White Blood Cell Counting Techniques in BirdsPablo LópezPas encore d'évaluation
- 8.sadvritta (Code of Conduct)Document47 pages8.sadvritta (Code of Conduct)Vanisha AnoepPas encore d'évaluation
- Dagger's EdgeDocument34 pagesDagger's EdgeShanikea RamsayPas encore d'évaluation
- Ch. 13 EyeDocument46 pagesCh. 13 Eyefatucha87Pas encore d'évaluation
- MicronutrientsDocument21 pagesMicronutrientsJohn Paolo OcampoPas encore d'évaluation
- Principles & Practice of First AidDocument298 pagesPrinciples & Practice of First AidJoshua100% (2)
- StomachDocument16 pagesStomachnevelle4667Pas encore d'évaluation
- COPD and Lower Respiratory Infection GuideDocument4 pagesCOPD and Lower Respiratory Infection GuideIch RamPas encore d'évaluation
- Principle of The Method Quality Control: Alkaline PicrateDocument1 pagePrinciple of The Method Quality Control: Alkaline PicrateRisqon Anjahiranda Adiputra100% (1)
- Medial Longitudinal FasciculusDocument5 pagesMedial Longitudinal FasciculussakuraleeshaoranPas encore d'évaluation
- 英文TG900series 8885 lowDocument4 pages英文TG900series 8885 lowJose L GuzCamPas encore d'évaluation
- Production and Characterization of Mushroom ChitosanDocument4 pagesProduction and Characterization of Mushroom ChitosanmicrokannanPas encore d'évaluation
- DLL SampleDocument6 pagesDLL SampleJenny Domincel PrudentePas encore d'évaluation
- Language and BrainDocument23 pagesLanguage and Brainalbino100% (1)
- Throwing RehabDocument16 pagesThrowing RehabSean GlynnPas encore d'évaluation
- Figure 1 Human Nervous System Source:courses - Lumenlearning.c Om/microbiology/chapter/anato My-Of-The-Nervous-SystemDocument14 pagesFigure 1 Human Nervous System Source:courses - Lumenlearning.c Om/microbiology/chapter/anato My-Of-The-Nervous-SystemShekaina Faith Cuizon LozadaPas encore d'évaluation
- 76) Book Chapter 2010Document11 pages76) Book Chapter 2010Giovanni MauroPas encore d'évaluation
- Module 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionDocument229 pagesModule 1. General and Special Questions of Clinical Laboratory Diagnostics Text Test QuestionA.h.MuradPas encore d'évaluation
- Nursing Care PlanDocument5 pagesNursing Care Planruggero07100% (2)
- Sarns Modular Perfusion System 8000: A Flexible, Dependable, and Cost-Efficient Modular Blood Pumping SystemDocument4 pagesSarns Modular Perfusion System 8000: A Flexible, Dependable, and Cost-Efficient Modular Blood Pumping SystemAdvancemicronics MedicalsystemsPas encore d'évaluation
- Defense Mechanisms of the GingivaDocument249 pagesDefense Mechanisms of the GingivaAssssssPas encore d'évaluation
- Individual Behaviour: Biographical CharacteristicsDocument15 pagesIndividual Behaviour: Biographical Characteristicsapi-3792827Pas encore d'évaluation
- Big Can Be Beautiful, TIVA in The ObeseDocument7 pagesBig Can Be Beautiful, TIVA in The ObeseHernán GiménezPas encore d'évaluation
- Skripsi Tanpa Pembahasan PDFDocument64 pagesSkripsi Tanpa Pembahasan PDFBillyDwiSaputraPas encore d'évaluation
- BioPsych - Reviewer (MIdterm Exam) - Chapter 1Document6 pagesBioPsych - Reviewer (MIdterm Exam) - Chapter 1Francis Xavier AlcazarPas encore d'évaluation
- Bioavailabilitas Per Oral: Tradition of Excellence Tradition of ExcellenceDocument63 pagesBioavailabilitas Per Oral: Tradition of Excellence Tradition of ExcellencemiftaPas encore d'évaluation
- Bone Marrow A Practical Manual (2011)Document212 pagesBone Marrow A Practical Manual (2011)Victor Lage de AraujoPas encore d'évaluation