Vous aimerez peut-être aussi
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Esrd ReportDocument3 pagesEsrd ReportAlwina May Parojinog BarlisanPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Room AP Ward Name Age/Sex WT DOB Old/New Diagnosis Ji Admit Ji ProgressDocument1 pageRoom AP Ward Name Age/Sex WT DOB Old/New Diagnosis Ji Admit Ji ProgressAlwina May Parojinog BarlisanPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- TB Case PresDocument5 pagesTB Case PresAlwina May Parojinog BarlisanPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- TB Case PresDocument5 pagesTB Case PresAlwina May Parojinog BarlisanPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- Chronic Obstructive Pulmonary DiseaseDocument4 pagesChronic Obstructive Pulmonary DiseaseAlwina May Parojinog BarlisanPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Pathophysiology of Colon CancerDocument1 pagePathophysiology of Colon CancerAlwina May Parojinog BarlisanPas encore d'évaluation
- 13 Management of DiabetesDocument8 pages13 Management of DiabetesAlwina May Parojinog BarlisanPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
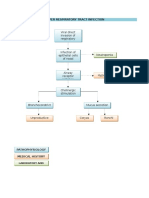
- Pathophysiology of Upper Respiratory InfectionsDocument1 pagePathophysiology of Upper Respiratory InfectionsAlwina May Parojinog BarlisanPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Different Surgical Options For Gastric Cancer Part 1Document6 pagesDifferent Surgical Options For Gastric Cancer Part 1Alwina May Parojinog BarlisanPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Vascular InjuryDocument17 pagesVascular InjuryAlwina May Parojinog BarlisanPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- Neck ChestDocument21 pagesNeck ChestAlwina May Parojinog BarlisanPas encore d'évaluation
- Skin Grafts and Skin SubstitutesDocument5 pagesSkin Grafts and Skin SubstitutesAlwina May Parojinog BarlisanPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Treatment ASDDocument7 pagesTreatment ASDAlwina May Parojinog BarlisanPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Theories DefinitionDocument2 pagesTheories DefinitionAlwina May Parojinog BarlisanPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Hypomagnesemia in NewbornDocument4 pagesHypomagnesemia in NewbornTheresa MendoncaPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Case Study-Infant With Fluid Imbalance08-10-KEYDocument3 pagesCase Study-Infant With Fluid Imbalance08-10-KEYreecolePas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- New India Cancer Guard PolicyDocument28 pagesNew India Cancer Guard PolicyumapPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- NCLEX Drug CardsDocument136 pagesNCLEX Drug CardsC Johnson100% (44)
- 047 Pathology MCQ ACEM Primary NeoplasiaDocument4 pages047 Pathology MCQ ACEM Primary NeoplasiaSa MaPas encore d'évaluation
- Lecture #5 - Circulatory DisturbanceDocument36 pagesLecture #5 - Circulatory DisturbanceEl Farouk100% (1)
- Perf. PeritonitisDocument5 pagesPerf. PeritonitisChiriţoiu AnamariaPas encore d'évaluation
- Texas Children's Hospital 5 Annual Advanced Practice Provider ConferenceDocument64 pagesTexas Children's Hospital 5 Annual Advanced Practice Provider ConferenceEngSabbaghPas encore d'évaluation
- How to Keep Your Heart HealthyDocument11 pagesHow to Keep Your Heart HealthyLarissa RevillaPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Blood TransfusionDocument30 pagesBlood TransfusionnoorgianilestariPas encore d'évaluation
- SKIN, HAIR, and NAILSDocument17 pagesSKIN, HAIR, and NAILSkhalidPas encore d'évaluation
- White Paper On Microbial Anti-Cancer Therapy and PDocument24 pagesWhite Paper On Microbial Anti-Cancer Therapy and PeullobaPas encore d'évaluation
- Carboxytherapy Experiences After Treating 280 PatientsDocument8 pagesCarboxytherapy Experiences After Treating 280 PatientsJuganu RussiaPas encore d'évaluation
- Left Thigh Pain: I. Chief Complaint/ Other ComplaintsDocument9 pagesLeft Thigh Pain: I. Chief Complaint/ Other ComplaintsDominic BristolPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Keratosis ObturansDocument12 pagesKeratosis ObturansRahma LuthfaPas encore d'évaluation
- Diagnostic Criteria For 298Document1 pageDiagnostic Criteria For 298Pradeep KumarPas encore d'évaluation
- 2010 Guideline AFDocument61 pages2010 Guideline AFyamtotlPas encore d'évaluation
- Sansure Biotech: Six Respiratory Pathogens Nucleic Acid Diagnostic Kit (PCR-Fluorescence Probing)Document4 pagesSansure Biotech: Six Respiratory Pathogens Nucleic Acid Diagnostic Kit (PCR-Fluorescence Probing)paulaPas encore d'évaluation
- Case Study PedsDocument11 pagesCase Study PedsGenesis Bicera100% (1)
- Gall Bladder CarcinomaDocument29 pagesGall Bladder CarcinomaUsman FarooqPas encore d'évaluation
- Telaah Kritis Artikel Terapi PZ 2020Document7 pagesTelaah Kritis Artikel Terapi PZ 2020dewi arifahniPas encore d'évaluation
- Appendicitis NCPDocument5 pagesAppendicitis NCPEarl Joseph DezaPas encore d'évaluation
- Anaesthesia For BurnsDocument51 pagesAnaesthesia For BurnsAnulatkPas encore d'évaluation
- Hypertension in Pregnancy (Pogs-Cpg)Document55 pagesHypertension in Pregnancy (Pogs-Cpg)Philip Piolo Fuego67% (3)
- Torticolis OdtDocument25 pagesTorticolis OdtAndreea CimpoiPas encore d'évaluation
- Upper Airway ObstructionDocument17 pagesUpper Airway ObstructionRai Hana100% (1)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFDocument16 pagesThe Joint Philippine Society of Gastroenterology and Philippine Society of Digestive Endoscopy Consensus Guidelines PDFaxxoPas encore d'évaluation
- Dialog AssignmentDocument4 pagesDialog AssignmentKitket Photografi & Cinematografi100% (1)
- CV SAMEEP - PathologistDocument7 pagesCV SAMEEP - PathologistMumtaj AnsariPas encore d'évaluation
- PART I: Vocabulary (20 Items - 4,0 Pts - 0,2 PTS/ Item) Questions 1-5Document5 pagesPART I: Vocabulary (20 Items - 4,0 Pts - 0,2 PTS/ Item) Questions 1-5Nguyễn TavirelPas encore d'évaluation