Vous aimerez peut-être aussi
- Congenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementD'EverandCongenital Hyperinsulinism: A Practical Guide to Diagnosis and ManagementDiva D. De León-CrutchlowPas encore d'évaluation
- AnencephalyDocument6 pagesAnencephalyMetta SariPas encore d'évaluation
- A Preterm Infant With Semilobar Holoprosencephaly and Hydrocephalus: A CaseDocument4 pagesA Preterm Infant With Semilobar Holoprosencephaly and Hydrocephalus: A CaseMuhd Idris Aizat AdamPas encore d'évaluation
- Umbilical Cord Hernias: Prenatal Diagnosis and Natural HistoryDocument4 pagesUmbilical Cord Hernias: Prenatal Diagnosis and Natural HistoryFriska GriffinPas encore d'évaluation
- Medical Hypotheses: J. Mercer, D. Erickson-Owens, R. SkovgaardDocument6 pagesMedical Hypotheses: J. Mercer, D. Erickson-Owens, R. SkovgaardRicardo MacíasPas encore d'évaluation
- Neonatal Seizures in Calabar: A Revisit: J. J. Udo, M. E. Eyong, M. U. Anah, I. S. Etuk, C. I. Uzomba and A. A. AsindiDocument7 pagesNeonatal Seizures in Calabar: A Revisit: J. J. Udo, M. E. Eyong, M. U. Anah, I. S. Etuk, C. I. Uzomba and A. A. Asindiambachew bizunehPas encore d'évaluation
- Case Study 1Document13 pagesCase Study 1Kiana TehraniPas encore d'évaluation
- Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument11 pagesIleal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenEmmanuelLeidiPas encore d'évaluation
- Ultrasound Features of Spermatic Cord Hydrocele in ChildrenDocument3 pagesUltrasound Features of Spermatic Cord Hydrocele in ChildrenEnricoFermihutagalungPas encore d'évaluation
- Finer, (1981) - Hypoxic-Ischemic Encephalopathy in Term Neonates Perinatal Factors and Outcome. The Journal of PediatricsDocument6 pagesFiner, (1981) - Hypoxic-Ischemic Encephalopathy in Term Neonates Perinatal Factors and Outcome. The Journal of PediatricsKatherine FernandezPas encore d'évaluation
- Case Report Tuberculous Otitis MediaDocument23 pagesCase Report Tuberculous Otitis MediahwelpPas encore d'évaluation
- Oropharyngealdysphagia Inchildren: Mechanism, Source, and ManagementDocument30 pagesOropharyngealdysphagia Inchildren: Mechanism, Source, and ManagementArif oktavianPas encore d'évaluation
- Neurologia NeonatalDocument7 pagesNeurologia NeonatalRoberto CongPas encore d'évaluation
- An Evaluation of The Effects of Hypertension During Pregnancy On Postpartum Hearing As Measured by Transient-Evoked Otoacoustic EmissionsDocument6 pagesAn Evaluation of The Effects of Hypertension During Pregnancy On Postpartum Hearing As Measured by Transient-Evoked Otoacoustic Emissionsbunyamin99Pas encore d'évaluation
- New Born Children With Encephalocele: Imedpub JournalsDocument4 pagesNew Born Children With Encephalocele: Imedpub Journalsglory haurissaPas encore d'évaluation
- Case 36-2004: A 23-Day-Old Infant With Hypospadias and Failure To ThriveDocument8 pagesCase 36-2004: A 23-Day-Old Infant With Hypospadias and Failure To ThriveGaniahUtamiPas encore d'évaluation
- Hirschsprung DiseaseDocument44 pagesHirschsprung DiseaseAhmad Abu KushPas encore d'évaluation
- Lancet Article PDFDocument5 pagesLancet Article PDFBrandy GarciaPas encore d'évaluation
- ANENCEPHALYDocument10 pagesANENCEPHALYSharmaine SimonPas encore d'évaluation
- Ileal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenDocument5 pagesIleal-Lymphoid-Nodular Hyperplasia, Non-Specific Colitis, and Pervasive Developmental Disorder in ChildrenAnonymous 7hW4aGPas encore d'évaluation
- Case Study On Intrauterine Fetal Demise (Final Draft)Document11 pagesCase Study On Intrauterine Fetal Demise (Final Draft)Anne Mosquite82% (11)
- Neural Tube DefectDocument8 pagesNeural Tube DefectReema Akberali nooraniPas encore d'évaluation
- Neonatal Hiatal Hernia - A Rare Case ReportDocument4 pagesNeonatal Hiatal Hernia - A Rare Case ReportAgus DarwiyantoPas encore d'évaluation
- Fetal Cystic Hygroma The Importance of Natural HistoryDocument7 pagesFetal Cystic Hygroma The Importance of Natural HistoryNGUYỄN XUÂN SangPas encore d'évaluation
- Pediatric Clinics of North America IIDocument54 pagesPediatric Clinics of North America IIkarenPas encore d'évaluation
- Pott's Puffy Tumor in A 12-Year-Old Boy: ReferencesDocument4 pagesPott's Puffy Tumor in A 12-Year-Old Boy: ReferencesssmasterPas encore d'évaluation
- Are Routine Cranial Ultrasounds Necessary in Premature Infants Greater Than 30 Weeks Gestation?Document5 pagesAre Routine Cranial Ultrasounds Necessary in Premature Infants Greater Than 30 Weeks Gestation?Wulan CerankPas encore d'évaluation
- Cerebral PalsyDocument7 pagesCerebral PalsyFernando Suarez ChumaceroPas encore d'évaluation
- Birth Asphycia and Cerebral Palsy Clinics Perinatology 2005Document16 pagesBirth Asphycia and Cerebral Palsy Clinics Perinatology 2005Sebastián Silva SotoPas encore d'évaluation
- University of Northern PhilippinesDocument6 pagesUniversity of Northern PhilippinesEliazar Alumbro Peniton Jr.Pas encore d'évaluation
- Comparison Between Small and Large Bowel Intussusception in ChildrenDocument3 pagesComparison Between Small and Large Bowel Intussusception in ChildrenParamartha KesumaPas encore d'évaluation
- Choanal AtresiaDocument8 pagesChoanal AtresiaCharmila Sari0% (1)
- Brainstem Auditory Function at Term in Preterm Babies With and Without Perinatal ComplicationsDocument6 pagesBrainstem Auditory Function at Term in Preterm Babies With and Without Perinatal ComplicationsRadianNasutionPas encore d'évaluation
- Vertigo: Perilymphatic Fistula-A Definitive and Curable Cause of Following Head TraumaDocument4 pagesVertigo: Perilymphatic Fistula-A Definitive and Curable Cause of Following Head TraumazobidaPas encore d'évaluation
- Middle Interhemisferic Variant HoloprosencaphalyDocument4 pagesMiddle Interhemisferic Variant HoloprosencaphalyAhmet Kürşad PoyrazPas encore d'évaluation
- Vomiting in A Neonate Dorothy Damore MDDocument5 pagesVomiting in A Neonate Dorothy Damore MDHanny RusliPas encore d'évaluation
- Pattern of Neonatal Seizures in Osogbo, South-Western NigeriaDocument4 pagesPattern of Neonatal Seizures in Osogbo, South-Western Nigeriaambachew bizunehPas encore d'évaluation
- Hearing Loss in Term Newborn Infants With Hypoxic-Ischemic Encephalopathy Treated With Therapeutic Hypothermia PDFDocument8 pagesHearing Loss in Term Newborn Infants With Hypoxic-Ischemic Encephalopathy Treated With Therapeutic Hypothermia PDFstefanp89Pas encore d'évaluation
- 631-Article Text-2378-1-10-20180830Document6 pages631-Article Text-2378-1-10-20180830azizhamoudPas encore d'évaluation
- AMS PublishedDocument4 pagesAMS PublishedAyanawPas encore d'évaluation
- CLINICAL PRESENTATION VinDocument54 pagesCLINICAL PRESENTATION VinVineetha ThachedathPas encore d'évaluation
- Lec 1Document52 pagesLec 1zainabd1964Pas encore d'évaluation
- Eroswr GWGRDocument12 pagesEroswr GWGRPrasetio Kristianto BudionoPas encore d'évaluation
- 216 FTPDocument8 pages216 FTPapi-289577018Pas encore d'évaluation
- Henoch Schonlein Purpura (IgA Vasculitis)Document15 pagesHenoch Schonlein Purpura (IgA Vasculitis)Emily Eresuma100% (1)
- A Schematic Approach To Hypotonia in Infancy: Une Démarche Schématique Envers L'hypotonie Pendant La Première EnfanceDocument4 pagesA Schematic Approach To Hypotonia in Infancy: Une Démarche Schématique Envers L'hypotonie Pendant La Première EnfanceRahul RaiPas encore d'évaluation
- 933 FullDocument9 pages933 FullGaurav MedikeriPas encore d'évaluation
- Case PresentationDocument34 pagesCase PresentationgpstPas encore d'évaluation
- The Control of Postpartum Haemorrhage With Intrauterine Foley CatheterDocument4 pagesThe Control of Postpartum Haemorrhage With Intrauterine Foley CatheterKien BuiPas encore d'évaluation
- Fetal Intracranial Hemorrhage: Is Minor Maternal Trauma A Possible Pathogenetic Factor?Document8 pagesFetal Intracranial Hemorrhage: Is Minor Maternal Trauma A Possible Pathogenetic Factor?Kareem AhmedPas encore d'évaluation
- Large, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumDocument5 pagesLarge, Solitary, Luteinized Follicle Cyst of Pregnancy and PuerperiumMade RusmanaPas encore d'évaluation
- Labial AdhesionsDocument2 pagesLabial AdhesionsLydia TsiaplePas encore d'évaluation
- JCM 11 05684 v2Document13 pagesJCM 11 05684 v2Qwerty AsdfghPas encore d'évaluation
- Brmedj00111 0029aDocument1 pageBrmedj00111 0029aapi-289577018Pas encore d'évaluation
- Neural Tube Defects and Folate: Case Far From Closed: ReviewsDocument8 pagesNeural Tube Defects and Folate: Case Far From Closed: ReviewsGeomar LaraPas encore d'évaluation
- Ciorba2019 PDFDocument6 pagesCiorba2019 PDFFiona ApriliaPas encore d'évaluation
- Articol 1Document7 pagesArticol 1nistor97Pas encore d'évaluation
- 393 FullDocument10 pages393 FullMateen ShukriPas encore d'évaluation
- Neonatal Resuscitation: Thomas E Wiswell MDDocument8 pagesNeonatal Resuscitation: Thomas E Wiswell MDm6000000Pas encore d'évaluation
- Medind - Nic.in Icb t05 I5 Icbt05i5p445Document4 pagesMedind - Nic.in Icb t05 I5 Icbt05i5p445Ester SibaraniPas encore d'évaluation
- Lab Report 1: Dna Extraction From Peripheral Blood Mononuclear Cells (PBMC)Document7 pagesLab Report 1: Dna Extraction From Peripheral Blood Mononuclear Cells (PBMC)Nida RidzuanPas encore d'évaluation
- Staphylococcus Aureus Biofilms Interfere With Macrophage AntimicrDocument175 pagesStaphylococcus Aureus Biofilms Interfere With Macrophage AntimicrshalusinhaPas encore d'évaluation
- 2019 32 Notifn Vet Asst SurgDocument26 pages2019 32 Notifn Vet Asst SurgThiru NavukarasuPas encore d'évaluation
- Flow Cytometry: Surface Markers and Beyond: Methods of Allergy and ImmunologyDocument10 pagesFlow Cytometry: Surface Markers and Beyond: Methods of Allergy and ImmunologyMunir AliPas encore d'évaluation
- Calcinosis Cutis Report of 4 CasesDocument2 pagesCalcinosis Cutis Report of 4 CasesEtty FaridaPas encore d'évaluation
- Antibodies To Watch in 2019: Hélène Kaplon & Janice M. ReichertDocument46 pagesAntibodies To Watch in 2019: Hélène Kaplon & Janice M. ReichertAjay KumarPas encore d'évaluation
- Review Article: Carbon Nanotubes: Applications in Pharmacy and MedicineDocument13 pagesReview Article: Carbon Nanotubes: Applications in Pharmacy and MedicineShrinivas KatkamwarPas encore d'évaluation
- The SOMATID - A Pleomorphic, Ultra-Microsopic Subcellular Living and Reproducing EntityDocument55 pagesThe SOMATID - A Pleomorphic, Ultra-Microsopic Subcellular Living and Reproducing EntityMarkMadMunkiPas encore d'évaluation
- Community Health Nursing Questions ADocument11 pagesCommunity Health Nursing Questions AFleur Jenne100% (1)
- Skin and Its AppendagesDocument3 pagesSkin and Its AppendagesMarchylle Faye JimenezPas encore d'évaluation
- WL7 Abstracts BookDocument1 514 pagesWL7 Abstracts BookJaison Enrique Torres PachecoPas encore d'évaluation
- What Really Causes High CholesterolDocument5 pagesWhat Really Causes High CholesterolsnickoletPas encore d'évaluation
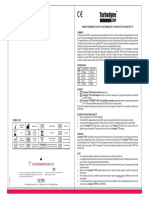
- Turbodyne: Tulip Diagnostics (P) LTDDocument2 pagesTurbodyne: Tulip Diagnostics (P) LTDMatibar RahmanPas encore d'évaluation
- Learning Activity Sheet in Science 10Document10 pagesLearning Activity Sheet in Science 10Sheee ShhheshPas encore d'évaluation
- Regulating The Cell Cycle: Lesson SummaryDocument7 pagesRegulating The Cell Cycle: Lesson SummaryKayPas encore d'évaluation
- IVMS Cell Biology and Pathology Flash Facts IDocument4 999 pagesIVMS Cell Biology and Pathology Flash Facts IMarc Imhotep Cray, M.D.0% (2)
- Cancer Cells Induce Metastasis-Supporting Neutrophil Extracellular DNA TrapsDocument13 pagesCancer Cells Induce Metastasis-Supporting Neutrophil Extracellular DNA TrapsJoe DaccachePas encore d'évaluation
- Early HumanDocument4 pagesEarly HumanPeem JatabutPas encore d'évaluation
- Activity and ExerciseDocument30 pagesActivity and ExerciseSIVA KRISHNA PRASAD ARJAPas encore d'évaluation
- Emma Holiday PediatricsDocument78 pagesEmma Holiday PediatricsRyan Franz100% (1)
- Managing Rheumatic and Musculoskeletal Diseases - Past, Present and FutureDocument6 pagesManaging Rheumatic and Musculoskeletal Diseases - Past, Present and FutureNICOLASPas encore d'évaluation
- Test Bank For Human Anatomy 5th Edition MariebDocument18 pagesTest Bank For Human Anatomy 5th Edition MariebSandra Brown100% (5)
- The Flesh and Bones of Medical PharmacologyDocument149 pagesThe Flesh and Bones of Medical PharmacologyBijay Gaurav100% (1)
- Immunology NotesDocument8 pagesImmunology NotesSumit Mukherjee100% (1)
- ASNC AND EANM Amyloidosis Practice Points WEBDocument12 pagesASNC AND EANM Amyloidosis Practice Points WEBElena FlorentinaPas encore d'évaluation
- B5 Lecture Slides (CMF) Folate AntagonistsDocument15 pagesB5 Lecture Slides (CMF) Folate AntagonistsZhen Yuan GaryPas encore d'évaluation
- 7 ZileDocument14 pages7 ZileSte Pa100% (1)
- Amniotic Fluid and ItDocument8 pagesAmniotic Fluid and ItSaman SarKoPas encore d'évaluation
- Ria ImmunoassayDocument10 pagesRia ImmunoassayDinkey SharmaPas encore d'évaluation
- The Obesity Code: Unlocking the Secrets of Weight LossD'EverandThe Obesity Code: Unlocking the Secrets of Weight LossÉvaluation : 4 sur 5 étoiles4/5 (5)
- By the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsD'EverandBy the Time You Read This: The Space between Cheslie's Smile and Mental Illness—Her Story in Her Own WordsPas encore d'évaluation
- Think This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeD'EverandThink This, Not That: 12 Mindshifts to Breakthrough Limiting Beliefs and Become Who You Were Born to BeÉvaluation : 2 sur 5 étoiles2/5 (1)
- The Age of Magical Overthinking: Notes on Modern IrrationalityD'EverandThe Age of Magical Overthinking: Notes on Modern IrrationalityÉvaluation : 4 sur 5 étoiles4/5 (24)
- The Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaD'EverandThe Body Keeps the Score by Bessel Van der Kolk, M.D. - Book Summary: Brain, Mind, and Body in the Healing of TraumaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Summary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisD'EverandSummary: Outlive: The Science and Art of Longevity by Peter Attia MD, With Bill Gifford: Key Takeaways, Summary & AnalysisÉvaluation : 4.5 sur 5 étoiles4.5/5 (42)
- Summary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedD'EverandSummary: The Psychology of Money: Timeless Lessons on Wealth, Greed, and Happiness by Morgan Housel: Key Takeaways, Summary & Analysis IncludedÉvaluation : 5 sur 5 étoiles5/5 (80)
- ADHD is Awesome: A Guide to (Mostly) Thriving with ADHDD'EverandADHD is Awesome: A Guide to (Mostly) Thriving with ADHDÉvaluation : 5 sur 5 étoiles5/5 (1)
- Self-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!D'EverandSelf-Care for Autistic People: 100+ Ways to Recharge, De-Stress, and Unmask!Évaluation : 5 sur 5 étoiles5/5 (1)
- Raising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsD'EverandRaising Mentally Strong Kids: How to Combine the Power of Neuroscience with Love and Logic to Grow Confident, Kind, Responsible, and Resilient Children and Young AdultsÉvaluation : 5 sur 5 étoiles5/5 (1)
- Outlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisD'EverandOutlive: The Science and Art of Longevity by Peter Attia: Key Takeaways, Summary & AnalysisÉvaluation : 4 sur 5 étoiles4/5 (1)
- The Comfort of Crows: A Backyard YearD'EverandThe Comfort of Crows: A Backyard YearÉvaluation : 4.5 sur 5 étoiles4.5/5 (23)
- Dark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.D'EverandDark Psychology & Manipulation: Discover How To Analyze People and Master Human Behaviour Using Emotional Influence Techniques, Body Language Secrets, Covert NLP, Speed Reading, and Hypnosis.Évaluation : 4.5 sur 5 étoiles4.5/5 (110)
- Gut: the new and revised Sunday Times bestsellerD'EverandGut: the new and revised Sunday Times bestsellerÉvaluation : 4 sur 5 étoiles4/5 (392)
- Why We Die: The New Science of Aging and the Quest for ImmortalityD'EverandWhy We Die: The New Science of Aging and the Quest for ImmortalityÉvaluation : 4 sur 5 étoiles4/5 (3)
- Raising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsD'EverandRaising Good Humans: A Mindful Guide to Breaking the Cycle of Reactive Parenting and Raising Kind, Confident KidsÉvaluation : 4.5 sur 5 étoiles4.5/5 (169)
- Cult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryD'EverandCult, A Love Story: Ten Years Inside a Canadian Cult and the Subsequent Long Road of RecoveryÉvaluation : 4 sur 5 étoiles4/5 (44)
- Mindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessD'EverandMindset by Carol S. Dweck - Book Summary: The New Psychology of SuccessÉvaluation : 4.5 sur 5 étoiles4.5/5 (328)
- The Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsD'EverandThe Ritual Effect: From Habit to Ritual, Harness the Surprising Power of Everyday ActionsÉvaluation : 3.5 sur 5 étoiles3.5/5 (3)
- When the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisD'EverandWhen the Body Says No by Gabor Maté: Key Takeaways, Summary & AnalysisÉvaluation : 3.5 sur 5 étoiles3.5/5 (2)
- Sleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningD'EverandSleep Stories for Adults: Overcome Insomnia and Find a Peaceful AwakeningÉvaluation : 4 sur 5 étoiles4/5 (3)
- Gut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)D'EverandGut: The Inside Story of Our Body's Most Underrated Organ (Revised Edition)Évaluation : 4 sur 5 étoiles4/5 (378)
- To Explain the World: The Discovery of Modern ScienceD'EverandTo Explain the World: The Discovery of Modern ScienceÉvaluation : 3.5 sur 5 étoiles3.5/5 (51)
- The Marshmallow Test: Mastering Self-ControlD'EverandThe Marshmallow Test: Mastering Self-ControlÉvaluation : 4.5 sur 5 étoiles4.5/5 (58)