Vous aimerez peut-être aussi
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- PDF Processed With Cutepdf Evaluation EditionDocument3 pagesPDF Processed With Cutepdf Evaluation EditionShyam SunderPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
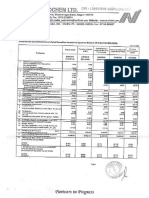
- Standalone Financial Results For March 31, 2016 (Result)Document11 pagesStandalone Financial Results For March 31, 2016 (Result)Shyam SunderPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Standalone Financial Results For September 30, 2016 (Result)Document3 pagesStandalone Financial Results For September 30, 2016 (Result)Shyam SunderPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Standalone Financial Results, Limited Review Report For June 30, 2016 (Result)Document3 pagesStandalone Financial Results, Limited Review Report For June 30, 2016 (Result)Shyam SunderPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Standalone Financial Results, Limited Review Report For September 30, 2016 (Result)Document4 pagesStandalone Financial Results, Limited Review Report For September 30, 2016 (Result)Shyam SunderPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Transcript of The Investors / Analysts Con Call (Company Update)Document15 pagesTranscript of The Investors / Analysts Con Call (Company Update)Shyam SunderPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Investor Presentation For December 31, 2016 (Company Update)Document27 pagesInvestor Presentation For December 31, 2016 (Company Update)Shyam SunderPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Standalone Financial Results, Limited Review Report For December 31, 2016 (Result)Document4 pagesStandalone Financial Results, Limited Review Report For December 31, 2016 (Result)Shyam SunderPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Judith Jarvis Thomson The Trolley Problem PDFDocument22 pagesJudith Jarvis Thomson The Trolley Problem PDFChirtu Ana-MariaPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Keeping You in Contact With Your CommunityDocument8 pagesKeeping You in Contact With Your CommunitySanaa PetersenPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- BMI - MediPlan - 250 - R7 - 11 - 1 - 21 - 1 ContratoDocument28 pagesBMI - MediPlan - 250 - R7 - 11 - 1 - 21 - 1 Contratoivantv2014Pas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Ethics of Organ DonationDocument19 pagesThe Ethics of Organ DonationJoslin Roz GalileaPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Research in Managerial Accounting 1. What Is The Malcolm Baldrige National Quality Award?Document4 pagesResearch in Managerial Accounting 1. What Is The Malcolm Baldrige National Quality Award?Jelay QuilatanPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- ReadingDocument13 pagesReadingQuỳnh Anh NguyễnPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Kidney Transplantation ReflectionDocument2 pagesKidney Transplantation Reflectionapi-523306558Pas encore d'évaluation
- Fortisian 5 MBDocument44 pagesFortisian 5 MBBadass BitchPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- KDIGO Transplantation GuidelinesDocument2 pagesKDIGO Transplantation GuidelinesSoteres VrachnesPas encore d'évaluation
- The Slave Formerly Known As Jane ForemanDocument133 pagesThe Slave Formerly Known As Jane Foremandholladay_1Pas encore d'évaluation
- Assignment Organ Donation and Role of NurseDocument10 pagesAssignment Organ Donation and Role of NurseParth VasavePas encore d'évaluation
- The Warrior May 2015Document23 pagesThe Warrior May 2015thewarrioronline_shsPas encore d'évaluation
- Biotransplant Inc.Document15 pagesBiotransplant Inc.Juan Manuel GonzalezPas encore d'évaluation
- Ethical IssuesDocument21 pagesEthical IssuesTriccie AbinojaPas encore d'évaluation
- KasaiDocument7 pagesKasaishalukiriPas encore d'évaluation
- Organ TransplantationDocument37 pagesOrgan TransplantationLaila Abdul100% (1)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Healing Kidney Failure NaturallyDocument56 pagesHealing Kidney Failure NaturallyGanesh Shankarram100% (2)
- Liver Transplantation in Adults - Patient Selection and Pretransplantation Evaluation - UpToDateDocument13 pagesLiver Transplantation in Adults - Patient Selection and Pretransplantation Evaluation - UpToDatematteoPas encore d'évaluation
- 2-Saglik Bilimleri Yokdil Deneme Aralik 2020 Akin Dil-136259Document24 pages2-Saglik Bilimleri Yokdil Deneme Aralik 2020 Akin Dil-136259MAHMUT KARANFİLPas encore d'évaluation
- OrganDocument391 pagesOrganmonimoy100% (1)
- Test 2: GRE Real 19Document8 pagesTest 2: GRE Real 19chiPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- The Seventh-Day Adventist Tradition: Religious Beliefs and Healthcare DecisionsDocument12 pagesThe Seventh-Day Adventist Tradition: Religious Beliefs and Healthcare Decisionsvani chelluriPas encore d'évaluation
- Term Paper 1Document7 pagesTerm Paper 1Romeo Macali Jr.Pas encore d'évaluation
- Human Organ Tranplantation ActDocument6 pagesHuman Organ Tranplantation ActFrank NobodPas encore d'évaluation
- Hla Unrelated DonorDocument2 pagesHla Unrelated Donorapi-410580205Pas encore d'évaluation
- Public Speaking Midterm (MOD)Document15 pagesPublic Speaking Midterm (MOD)Johnny OliverPas encore d'évaluation
- IMA Monthly Report Form JulyDocument4 pagesIMA Monthly Report Form JulyInternetStudioPas encore d'évaluation
- Final Dont Get High PDFDocument268 pagesFinal Dont Get High PDFSteve PetersonPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Medica Hospital PDFDocument131 pagesMedica Hospital PDFAdarsh ClinicPas encore d'évaluation
- House Hearing, 114TH Congress - Organ Harvesting: An Examination of A Brutal PracticeDocument64 pagesHouse Hearing, 114TH Congress - Organ Harvesting: An Examination of A Brutal PracticeScribd Government DocsPas encore d'évaluation