Vous aimerez peut-être aussi
- Cpe 15 097Document4 pagesCpe 15 097Syifa MustikaPas encore d'évaluation
- Gastroenterology2 CONFERENCESDocument1 pageGastroenterology2 CONFERENCESSyifa MustikaPas encore d'évaluation
- Gut Microbiome and Aging Physiological and MechaniDocument20 pagesGut Microbiome and Aging Physiological and MechaniSyifa MustikaPas encore d'évaluation
- BCLC Staging System: Stage 0 PST 0, Child-Pugh A, Okuda 1Document1 pageBCLC Staging System: Stage 0 PST 0, Child-Pugh A, Okuda 1Syifa MustikaPas encore d'évaluation
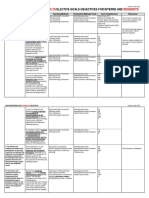
- Consults Residents: Gastroenterology /elective Goals-Objectives For Interns andDocument2 pagesConsults Residents: Gastroenterology /elective Goals-Objectives For Interns andSyifa MustikaPas encore d'évaluation
- Mucosal Immune System, & The Role of Iga in The Mucosal ImmunityDocument6 pagesMucosal Immune System, & The Role of Iga in The Mucosal ImmunitySyifa MustikaPas encore d'évaluation
- Poison 1Document24 pagesPoison 1Scott LarsonPas encore d'évaluation
- UEG Week Vienna 2014 - Abstract Issue PDFDocument661 pagesUEG Week Vienna 2014 - Abstract Issue PDFSyifa MustikaPas encore d'évaluation
- Mna Mini EnglishDocument1 pageMna Mini EnglishSyifa MustikaPas encore d'évaluation
- Universal PrecautionDocument39 pagesUniversal PrecautionSyifa MustikaPas encore d'évaluation
- Nutritional AssessmentDocument27 pagesNutritional AssessmentSyifa MustikaPas encore d'évaluation
- Argon Plasma Coagulation PDFDocument4 pagesArgon Plasma Coagulation PDFSyifa MustikaPas encore d'évaluation
- Energy Requirements For AdultsDocument3 pagesEnergy Requirements For AdultsSyifa MustikaPas encore d'évaluation
- Intrferon 2bDocument9 pagesIntrferon 2bSyifa MustikaPas encore d'évaluation
- Pharmakokinetic Protein TherpeuticsDocument29 pagesPharmakokinetic Protein TherpeuticsSyifa MustikaPas encore d'évaluation
- Code of Conduct Farmasi PDFDocument38 pagesCode of Conduct Farmasi PDFSyifa MustikaPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Obstetric by 10 Teachers Chapter 8Document25 pagesObstetric by 10 Teachers Chapter 8FerasPas encore d'évaluation
- AcromegalyDocument14 pagesAcromegalyapi-312256950Pas encore d'évaluation
- 14-15 Peds Key Word Analysis NbomeDocument3 pages14-15 Peds Key Word Analysis NbomeChris Dubuque0% (1)
- Nursing Care Plan Breast-CancerDocument2 pagesNursing Care Plan Breast-CancerGreg Llandelar100% (2)
- Journal of Learning InsightsDocument12 pagesJournal of Learning InsightsJisel-Apple Bulan100% (2)
- Abstrak Medika Mentosa PDFDocument3 pagesAbstrak Medika Mentosa PDFpawiroPas encore d'évaluation
- ProposalDocument3 pagesProposalMacky F ColasitoPas encore d'évaluation
- Endocrine System DisordersDocument83 pagesEndocrine System DisordersJerilee SoCute Watts0% (1)
- ENT Deferential Diagnosis MEDADDocument22 pagesENT Deferential Diagnosis MEDADReham AshourPas encore d'évaluation
- Paediatric Protocols 3rd Edition 2012.Document693 pagesPaediatric Protocols 3rd Edition 2012.Sumita Muniandy67% (3)
- CA EndometriumDocument46 pagesCA EndometriumNovianaHartikasariPas encore d'évaluation
- Phytochemical Composition of Sargassum Polycystum C. Agardh and SargassumDocument5 pagesPhytochemical Composition of Sargassum Polycystum C. Agardh and SargassumWaraNovekaPas encore d'évaluation
- Palmer Set 5Document7 pagesPalmer Set 5Jes CmtPas encore d'évaluation
- RRLDocument7 pagesRRLRomesor ApolPas encore d'évaluation
- Research CHAPTER 1Document2 pagesResearch CHAPTER 1Britnee Shantelle BayangPas encore d'évaluation
- Assessment of Nutritional Status of Children Under Five Years of Age in Rural NepalDocument3 pagesAssessment of Nutritional Status of Children Under Five Years of Age in Rural NepalAnna Marie Santos100% (1)
- IAEA Planning National Radiotherapy Services - A Practical Tool PDFDocument100 pagesIAEA Planning National Radiotherapy Services - A Practical Tool PDFTomás Alexander Alvis MenachoPas encore d'évaluation
- Gastric Surgery MCQDocument6 pagesGastric Surgery MCQSajag GuptaPas encore d'évaluation
- A Review of Biopsy in Dentistry: Principles, Techniques, and ConsiderationsDocument8 pagesA Review of Biopsy in Dentistry: Principles, Techniques, and ConsiderationsDeepak KumarPas encore d'évaluation
- Genetically Modified FoodDocument10 pagesGenetically Modified FoodRafia ShabbirPas encore d'évaluation
- Total Glossectomy For Tongue CancerDocument10 pagesTotal Glossectomy For Tongue CancerRajan KarmakarPas encore d'évaluation
- Smoothelin (R4A) - CM - MAN - EN - IVD - 1.0 PDFDocument5 pagesSmoothelin (R4A) - CM - MAN - EN - IVD - 1.0 PDFOlteanu Gheorghe-EmilianPas encore d'évaluation
- Script Ma'am PrescyDocument9 pagesScript Ma'am PrescyErl Joseph G. EvangelioPas encore d'évaluation
- Wild Foods For Wise Women by Susun WeedDocument6 pagesWild Foods For Wise Women by Susun Weedclaricecaps100% (1)
- Nasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyDocument4 pagesNasal Polyp Nasa Arsha Management Through Ayurveda A Single Case StudyEditor IJTSRDPas encore d'évaluation
- Cytology of Bone Fine Needle Aspiration BiopsyDocument11 pagesCytology of Bone Fine Needle Aspiration BiopsyRavi MehrotraPas encore d'évaluation
- Dr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDocument26 pagesDr. S.K. Haldar's Lectures On Industrial Health For AFIH Students - Occu. Lung Dis Asbestosis Silicosis ByssinosisDr. Prakash Kulkarni100% (2)
- DM OAD 14 - RevDocument36 pagesDM OAD 14 - RevAri AsriniPas encore d'évaluation
- Juvenile Idiopathic ArthritisDocument52 pagesJuvenile Idiopathic ArthritishasanajPas encore d'évaluation
- Section A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Document13 pagesSection A Multiple Choice Questions Gynaecology: Prepared by Da Roux Barrett Class of 2014Sheldon FerronPas encore d'évaluation