Vous aimerez peut-être aussi
- Comentário 1 Ao TA 90 - Henry MullerDocument4 pagesComentário 1 Ao TA 90 - Henry MullerRodrigo Barros GewehrPas encore d'évaluation
- Comentário 3 Ao TA 85 - Henry MullerDocument4 pagesComentário 3 Ao TA 85 - Henry MullerRodrigo Barros GewehrPas encore d'évaluation
- Comentário 3 Ao TA 90 - PatlavskyiDocument3 pagesComentário 3 Ao TA 90 - PatlavskyiRodrigo Barros GewehrPas encore d'évaluation
- Comentário 5 Ao TA 85 - Henry MullerDocument4 pagesComentário 5 Ao TA 85 - Henry MullerRodrigo Barros GewehrPas encore d'évaluation
- Derrida - HostipitalityDocument16 pagesDerrida - Hostipitalitysanchezmelado100% (1)
- The Lankavatara Sutra. A Mahayana TextDocument182 pagesThe Lankavatara Sutra. A Mahayana TextRodrigo Barros GewehrPas encore d'évaluation
- JWH-Sunyata and KenosisDocument19 pagesJWH-Sunyata and KenosisTimothy Smith100% (1)
- Aikido InsightsDocument16 pagesAikido InsightsRodrigo Barros GewehrPas encore d'évaluation
- Guba - Competing Paradigms in Qualitative ResearchDocument13 pagesGuba - Competing Paradigms in Qualitative ResearchRodrigo Barros GewehrPas encore d'évaluation
- Aikido InsightsDocument16 pagesAikido InsightsRodrigo Barros GewehrPas encore d'évaluation
- Biu Sante 74473Document290 pagesBiu Sante 74473Rodrigo Barros GewehrPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Justness and Sincerity 3-16-09Document5 pagesJustness and Sincerity 3-16-09Jayvee Lansangan100% (1)
- State - Politics and Economy of Rajasthan Volume-7Document23 pagesState - Politics and Economy of Rajasthan Volume-7abhilasha raoPas encore d'évaluation
- Agenda of The 107th Regular SessionDocument82 pagesAgenda of The 107th Regular SessionCdeoCityCouncilPas encore d'évaluation
- Marriage, Past and Present: A Debate Between Robert Bruffault and Bronislaw MalinowskiDocument104 pagesMarriage, Past and Present: A Debate Between Robert Bruffault and Bronislaw Malinowskilithren100% (1)
- Ifá InitiationDocument10 pagesIfá InitiationHazel83% (6)
- Habermas Public SphereDocument4 pagesHabermas Public SphereLarisa Elena Spirea100% (1)
- 컴인잉 시험Document2 pages컴인잉 시험멜로디Pas encore d'évaluation
- Jews N The Neo Cons-Heilbrunn & McdonaldDocument18 pagesJews N The Neo Cons-Heilbrunn & McdonaldDilip SenguptaPas encore d'évaluation
- Maysir 1Document19 pagesMaysir 1farhan israrPas encore d'évaluation
- Notes & Questions - CivicsDocument15 pagesNotes & Questions - CivicsvibhorxpandeyPas encore d'évaluation
- 00001t TifDocument342 pages00001t TifjamesPas encore d'évaluation
- AutonomyDocument6 pagesAutonomyShekel SibalaPas encore d'évaluation
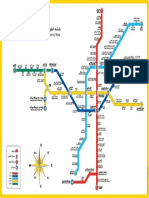
- Tehran Urban & Suburban Railway (Metro) Map: TajrishDocument1 pageTehran Urban & Suburban Railway (Metro) Map: TajrishthrashmetalerPas encore d'évaluation
- Malala Fahrenheit 451-2Document6 pagesMalala Fahrenheit 451-2api-285642057Pas encore d'évaluation
- The Anarchist PerilDocument296 pagesThe Anarchist Perilkolokotronis1770Pas encore d'évaluation
- H CSRDocument2 pagesH CSRLuvkush RulesPas encore d'évaluation
- Susi Vs RazonDocument1 pageSusi Vs RazonGladys BantilanPas encore d'évaluation
- Racial Identities Revisited - Toni Morrison's - Recitatif.Document13 pagesRacial Identities Revisited - Toni Morrison's - Recitatif.Ryan WilliamsPas encore d'évaluation
- Constructing A Bridge PDFDocument468 pagesConstructing A Bridge PDFstavros_stergPas encore d'évaluation
- Evaluate The View That Devolution Has Been A Success. (30) Politics Explained Essay PlanDocument5 pagesEvaluate The View That Devolution Has Been A Success. (30) Politics Explained Essay PlanlivphilbinPas encore d'évaluation
- China's Belt and Road Initiative and Its Implications For Global DevelopmentDocument28 pagesChina's Belt and Road Initiative and Its Implications For Global DevelopmentjayaravinthPas encore d'évaluation
- The Free Movement of Goods in The Europe PDFDocument17 pagesThe Free Movement of Goods in The Europe PDFSheroyaPas encore d'évaluation
- Governance and Public Policy in The UKDocument31 pagesGovernance and Public Policy in The UKDeimante BlikertaitePas encore d'évaluation
- John Locke Gen GoDocument11 pagesJohn Locke Gen GoragusakaPas encore d'évaluation
- Second Floor Reflected Ceiling Plan: LegendDocument1 pageSecond Floor Reflected Ceiling Plan: Legendaceboy_17Pas encore d'évaluation
- Opinion - : How Progressives Lost The 'Woke' Narrative - and What They Can Do To Reclaim It From The Right-WingDocument4 pagesOpinion - : How Progressives Lost The 'Woke' Narrative - and What They Can Do To Reclaim It From The Right-WingsiesmannPas encore d'évaluation
- Final-Final-Thesis 2Document74 pagesFinal-Final-Thesis 2Daniel DimanahanPas encore d'évaluation
- AP Euro Test Chapters 13-17Document25 pagesAP Euro Test Chapters 13-17Hilda WilliamsPas encore d'évaluation
- ST Paul Vs AnchetaDocument2 pagesST Paul Vs AnchetaAlan GultiaPas encore d'évaluation
- Water Org ResourcesDocument17 pagesWater Org ResourcesAndree Moore-MullinsPas encore d'évaluation