Vous aimerez peut-être aussi
- English Activity (Yoga Eka Pradana)Document2 pagesEnglish Activity (Yoga Eka Pradana)fikriPas encore d'évaluation
- 58 PDFDocument12 pages58 PDFSandri YaningsihPas encore d'évaluation
- Rasubala, Kumaat, Mulyadi 2017Document10 pagesRasubala, Kumaat, Mulyadi 2017Mohd Yanuar SaifudinPas encore d'évaluation
- 5179 16059 1 PBDocument11 pages5179 16059 1 PBfikriPas encore d'évaluation
- Perbanyakan in Vitro Dan Induksi Akumula 2Document10 pagesPerbanyakan in Vitro Dan Induksi Akumula 2fikriPas encore d'évaluation
- PDFDocument14 pagesPDFfikriPas encore d'évaluation
- Tema "Increasing Emergency Nurcing Skills Nursing ForDocument1 pageTema "Increasing Emergency Nurcing Skills Nursing ForfikriPas encore d'évaluation
- English Activity (Yoga Eka Pradana)Document2 pagesEnglish Activity (Yoga Eka Pradana)fikriPas encore d'évaluation
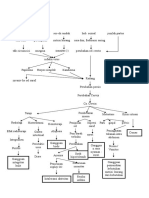
- Pathway CA ServiksDocument1 pagePathway CA ServiksfikriPas encore d'évaluation
- JAH3 5 E003019Document25 pagesJAH3 5 E003019fikriPas encore d'évaluation
- Ni Hms 540911Document17 pagesNi Hms 540911fikriPas encore d'évaluation
- 5179 16059 1 PBDocument11 pages5179 16059 1 PBfikriPas encore d'évaluation
- Vol.20 No.2 6 PDFDocument7 pagesVol.20 No.2 6 PDFfikriPas encore d'évaluation
- 6123 10036 1 SMDocument11 pages6123 10036 1 SMfikriPas encore d'évaluation
- 422 2016 Article 682Document26 pages422 2016 Article 682fikriPas encore d'évaluation
- 112233Document14 pages112233fikriPas encore d'évaluation
- JCDR 10 LC16Document5 pagesJCDR 10 LC16fikriPas encore d'évaluation
- Hubungan Antara Kekerasan Emosional Pada Anak Terhadap Kecenderungan Kenakalan RemajaDocument9 pagesHubungan Antara Kekerasan Emosional Pada Anak Terhadap Kecenderungan Kenakalan RemajafikriPas encore d'évaluation
- Ni Hms 526668Document23 pagesNi Hms 526668fikriPas encore d'évaluation
- Jurnal Maternity 5 PDFDocument1 pageJurnal Maternity 5 PDFfikriPas encore d'évaluation
- Jurnal Maternity 4Document9 pagesJurnal Maternity 4fikriPas encore d'évaluation
- Jurnal AromateraphyDocument30 pagesJurnal AromateraphyfikriPas encore d'évaluation
- Jurnal AromateraphyDocument30 pagesJurnal AromateraphyfikriPas encore d'évaluation
- Jurnal Maternitas 2Document21 pagesJurnal Maternitas 2fikriPas encore d'évaluation
- Jurnal Maternity 5Document1 pageJurnal Maternity 5fikriPas encore d'évaluation
- Jurnal Meternety Muhammad FikriyadiDocument6 pagesJurnal Meternety Muhammad FikriyadifikriPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Strategic ManagementDocument46 pagesStrategic ManagementWaseque Uddin Ahmed100% (2)
- The Clinical Practice of Neurological and Neurosurgical NursingDocument790 pagesThe Clinical Practice of Neurological and Neurosurgical NursingAllicia PutriPas encore d'évaluation
- Vein Visualization Using Near Infrared (NIR) Vein Finder - Pages 213-220Document8 pagesVein Visualization Using Near Infrared (NIR) Vein Finder - Pages 213-220Văn Hiền NguyễnPas encore d'évaluation
- Session Plan SampleDocument2 pagesSession Plan SampleNette de Guzman100% (2)
- Introduction To Home VisitingDocument27 pagesIntroduction To Home VisitingAFTAB H. ABBASIPas encore d'évaluation
- Nursing History FormatDocument5 pagesNursing History FormatMira AurumtinPas encore d'évaluation
- Taryn ZadunayskiDocument2 pagesTaryn Zadunayskiapi-278580762Pas encore d'évaluation
- Family Health Nursing and Community OrganizingDocument16 pagesFamily Health Nursing and Community OrganizingKimberly Louise LopezPas encore d'évaluation
- Quizlet PDFDocument4 pagesQuizlet PDFsgkismetPas encore d'évaluation
- Varcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple ChoiceDocument17 pagesVarcarolis: Essentials of Psychiatric Mental Health Nursing: Test Bank Chapter 10: Personality Disorders Multiple Choiceyaneidys perezPas encore d'évaluation
- Hallares ResumeDocument17 pagesHallares ResumeJacky Delima RNPas encore d'évaluation
- MC 2 - BiochemistryDocument8 pagesMC 2 - BiochemistryChelleyOllitroPas encore d'évaluation
- Shemeka Leonard Resume 2023Document3 pagesShemeka Leonard Resume 2023api-577750864Pas encore d'évaluation
- Hospital PlanningDocument24 pagesHospital PlanningDees_24Pas encore d'évaluation
- App LetterDocument4 pagesApp Letterjayson789Pas encore d'évaluation
- ObjectivesDocument2 pagesObjectivesAmy RamirezPas encore d'évaluation
- Yale School of Nursing Simulation Lab: WordsDocument1 pageYale School of Nursing Simulation Lab: WordsHartford CourantPas encore d'évaluation
- Compilation of Reviewer For Fundamentals of Nursing PDF FreeDocument49 pagesCompilation of Reviewer For Fundamentals of Nursing PDF FreeTyler VintPas encore d'évaluation
- Helen FairchildDocument3 pagesHelen FairchildSariiPas encore d'évaluation
- Pita Cyrel R. Activity 7Document5 pagesPita Cyrel R. Activity 7Lucky Lynn AbreraPas encore d'évaluation
- King's Goal Attainment TheoryDocument76 pagesKing's Goal Attainment TheoryJessica Christel Maglalang100% (3)
- Curriculum Vitae For Mrs Alita Gloria MpingaDocument9 pagesCurriculum Vitae For Mrs Alita Gloria Mpingaalita ngomanePas encore d'évaluation
- Nursing Home Visitation GuidanceDocument9 pagesNursing Home Visitation GuidanceNational Content DeskPas encore d'évaluation
- The role of Clinical Supervisors in interprofessional student educationDocument52 pagesThe role of Clinical Supervisors in interprofessional student educationDwi NopriyantoPas encore d'évaluation
- Sarah Perry Resume 5Document2 pagesSarah Perry Resume 5api-635690065Pas encore d'évaluation
- 4 - Staffing & ScheduleDocument12 pages4 - Staffing & Scheduleمحمد حسنPas encore d'évaluation
- Susan KleimanDocument4 pagesSusan KleimanJayson CatarajaPas encore d'évaluation
- CERTIFICATE FOR NURSING EDUCATION - Pdftoword PDFDocument6 pagesCERTIFICATE FOR NURSING EDUCATION - Pdftoword PDFSAYMABANUPas encore d'évaluation
- HNU Today Spring 2018 WEBDocument15 pagesHNU Today Spring 2018 WEBHoly Names UniversityPas encore d'évaluation
- Code of Good Governance For The Professions in The PhilippinesDocument3 pagesCode of Good Governance For The Professions in The Philippinesjanna mae patriarcaPas encore d'évaluation