Vous aimerez peut-être aussi
- APA - DSM 5 Depression Bereavement Exclusion PDFDocument2 pagesAPA - DSM 5 Depression Bereavement Exclusion PDFDaniel NgPas encore d'évaluation
- Approach: A. How The Kidney Handle The Proteins?Document9 pagesApproach: A. How The Kidney Handle The Proteins?Rashed ShatnawiPas encore d'évaluation
- Krisis HipertensiDocument12 pagesKrisis HipertensiDani NursePas encore d'évaluation
- Illness Biomagnetism TreatmentDocument3 pagesIllness Biomagnetism TreatmentSilvia Arias100% (2)
- Necrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandNecrotizing Fasciitis, (Flesh Eating Disease) A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- A Simple Guide to Stroke, (Cerebrovascular Infarction) Diagnosis, Treatment and Related ConditionsD'EverandA Simple Guide to Stroke, (Cerebrovascular Infarction) Diagnosis, Treatment and Related ConditionsPas encore d'évaluation
- Clinical Instructors Precepting Handbook 1516Document30 pagesClinical Instructors Precepting Handbook 1516Mônica ScattolinPas encore d'évaluation
- Pediatric Cardio-Respiratory AssessmentDocument9 pagesPediatric Cardio-Respiratory AssessmentRicky SpideyPas encore d'évaluation
- Childhood Obesity PowerPointDocument28 pagesChildhood Obesity PowerPointkbschulzPas encore d'évaluation
- At The DOCTOR Dialogues and Vocabulary ListDocument12 pagesAt The DOCTOR Dialogues and Vocabulary ListMax Tapia CastilloPas encore d'évaluation
- NCSBN - Pharmacology and ParenteralDocument36 pagesNCSBN - Pharmacology and ParenteralKarissa May Cortez92% (12)
- Comparison of Agarose Gel Serum Protein Electrophoresis and Immunofixation With Capillary Electrophoresis and ImmunotypingDocument96 pagesComparison of Agarose Gel Serum Protein Electrophoresis and Immunofixation With Capillary Electrophoresis and ImmunotypingZia Uddin75% (8)
- Differential Diagnosis of Valvular Heart DiseaseDocument10 pagesDifferential Diagnosis of Valvular Heart DiseaseAbhisek ChatterjeePas encore d'évaluation
- Closed Tibia and Fibula Fractures in 44-Year-Old Male PatientDocument25 pagesClosed Tibia and Fibula Fractures in 44-Year-Old Male Patientleonard0% (1)
- HEMODIALYSISDocument108 pagesHEMODIALYSISDan™100% (2)
- Basic Ecg 2016Document75 pagesBasic Ecg 2016api-284503860Pas encore d'évaluation
- Patient Data Sheet: General Appearance: RespiratoryDocument5 pagesPatient Data Sheet: General Appearance: RespiratoryAshley SutherlandPas encore d'évaluation
- HypertensionDocument19 pagesHypertensionmr_coolz282344Pas encore d'évaluation
- Module 11 Rational Cloze Drilling ExercisesDocument9 pagesModule 11 Rational Cloze Drilling Exercisesperagas0% (1)
- Fluid & Electrolyte Review: Organs, IV Solutions, ConditionsDocument2 pagesFluid & Electrolyte Review: Organs, IV Solutions, ConditionsteabagmanPas encore d'évaluation
- Torsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsD'EverandTorsade De Pointes, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsPas encore d'évaluation
- Morning Report: Jawaria K. Alam, MD/PGY3Document20 pagesMorning Report: Jawaria K. Alam, MD/PGY3Emily EresumaPas encore d'évaluation
- Assesment Chest PainDocument9 pagesAssesment Chest PainIpar Day100% (2)
- What Is HyperlipidemiaDocument9 pagesWhat Is Hyperlipidemiaichanara100% (2)
- Brain Gate ReportDocument31 pagesBrain Gate ReportRahul Bansal50% (4)
- Arm Sling Osce - by DR ShaliniDocument3 pagesArm Sling Osce - by DR ShaliniShalini ShanmugalingamPas encore d'évaluation
- Colchão Termico GaymarDocument84 pagesColchão Termico GaymarJoctã Dos Anjos SilvaPas encore d'évaluation
- Septic ShockDocument11 pagesSeptic ShockJonna Mae Agcaoili SalameroPas encore d'évaluation
- Seizures in ChildrenDocument21 pagesSeizures in ChildrenTera SurbaktiPas encore d'évaluation
- Status Asthmaticus in ChildrenDocument76 pagesStatus Asthmaticus in ChildrenJesterCruzPas encore d'évaluation
- Respiratory Disorders in PediatricsDocument11 pagesRespiratory Disorders in PediatricsMateo Geoff100% (1)
- Hemodialysis AssessmentDocument38 pagesHemodialysis AssessmentIan LelisPas encore d'évaluation
- Differential DiagnosisDocument5 pagesDifferential DiagnosisChristie LucasPas encore d'évaluation
- Pediatric Shock: A Guide to Identification, Classification and Initial ManagementDocument20 pagesPediatric Shock: A Guide to Identification, Classification and Initial ManagementvgmanjunathPas encore d'évaluation
- Abdominal DistentionDocument6 pagesAbdominal DistentionDumapis RichardPas encore d'évaluation
- Ventricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsD'EverandVentricular Septal Defect, A Simple Guide To The Condition, Treatment And Related ConditionsPas encore d'évaluation
- SLMC GC Ipch Osoe (Age) Oct 2019Document4 pagesSLMC GC Ipch Osoe (Age) Oct 2019Alvin FlorentinoPas encore d'évaluation
- Turkey Book 03 Internal Medicine PDFDocument47 pagesTurkey Book 03 Internal Medicine PDFPreaisPas encore d'évaluation
- Nur 111 Session 6 Sas 1Document12 pagesNur 111 Session 6 Sas 1Zzimply Tri Sha UmaliPas encore d'évaluation
- Organ DonationDocument9 pagesOrgan DonationAravindan Sundar100% (1)
- Uncovering an Uncommon Cause of PsychosisDocument2 pagesUncovering an Uncommon Cause of PsychosissavinaumarPas encore d'évaluation
- BronchiolitisDocument24 pagesBronchiolitisCristiana MunteanPas encore d'évaluation
- Dka GuidelineDocument16 pagesDka GuidelineGhada HusseinPas encore d'évaluation
- Wound ManagementDocument33 pagesWound ManagementDeSi BiLLaPas encore d'évaluation
- Valedictory Address of Kenneth Isaiah IDocument10 pagesValedictory Address of Kenneth Isaiah IJephte EleginoPas encore d'évaluation
- OSCE: Problem Focused HPI AbdomenDocument6 pagesOSCE: Problem Focused HPI AbdomenZagros Motamed100% (1)
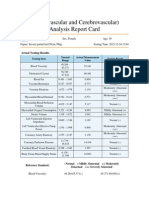
- Cardiovascular and CerebrovascularDocument6 pagesCardiovascular and CerebrovascularJoshelle B. Bancilo0% (1)
- Check Unit 556 December Digestive PDFDocument33 pagesCheck Unit 556 December Digestive PDFdragon66Pas encore d'évaluation
- Cannulation TrainingGuideDocument28 pagesCannulation TrainingGuideKavidu Keshan100% (1)
- Assessing Fetal and Maternal Health: Prenatal Care: Health Promotion During PregnancyDocument8 pagesAssessing Fetal and Maternal Health: Prenatal Care: Health Promotion During PregnancyMIKAELA DAVIDPas encore d'évaluation
- Assignmen 1 AnswersDocument3 pagesAssignmen 1 AnswersAlasl BobyPas encore d'évaluation
- Pediatric Hematology LectureDocument84 pagesPediatric Hematology LectureloitaPas encore d'évaluation
- Chapter 52 Endocrine Disorders Unit 1Document55 pagesChapter 52 Endocrine Disorders Unit 1Glory Mimi100% (1)
- K7 - Supraventricular Tachycardia (SVT)Document44 pagesK7 - Supraventricular Tachycardia (SVT)Zikri Putra Lan LubisPas encore d'évaluation
- Reye's SyndromeDocument11 pagesReye's SyndromeChristine Go100% (1)
- Managing Angina: AHA Guidelines on Diagnosis and TreatmentDocument96 pagesManaging Angina: AHA Guidelines on Diagnosis and TreatmentJaymica Laggui DacquilPas encore d'évaluation
- Mock Record B-1-2-Well Child VisitsDocument4 pagesMock Record B-1-2-Well Child VisitsaelteePas encore d'évaluation
- Delirium Pre-Test QuestionsDocument8 pagesDelirium Pre-Test QuestionsyohanesPas encore d'évaluation
- OSCE Reasoning and ConditionsDocument111 pagesOSCE Reasoning and ConditionsWiCKieWiCKPas encore d'évaluation
- Abdominal Swelling + AscitesDocument29 pagesAbdominal Swelling + AscitesDevina CiayadiPas encore d'évaluation
- Clinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephDocument15 pagesClinical Portfolio Name: Armeen Amin ENROLLMENT NO. 4-4/2019/001 BSCN Year Ii Group A Faculty Name: Ms. Roma JosephArmeen AminPas encore d'évaluation
- WWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Document5 pagesWWW - Qworld.co - in A-Z Disease List For NEETPG: IF Vit B Megaloblastic Anemia)Qworld100% (1)
- Vitamin B12 Deficiency and A Patient Case StudyDocument36 pagesVitamin B12 Deficiency and A Patient Case Studynherm6425100% (1)
- Pain Assessment in The Critically Ill Adult - Recent Evidence and New Trends PDFDocument11 pagesPain Assessment in The Critically Ill Adult - Recent Evidence and New Trends PDFSayonara BarbosaPas encore d'évaluation
- Exam 3 pathophysiology Cancer growth types and characteristicsDocument7 pagesExam 3 pathophysiology Cancer growth types and characteristicsmenickel3Pas encore d'évaluation
- Paediatric Septic Shock ManagementDocument37 pagesPaediatric Septic Shock ManagementJauhari DesloPas encore d'évaluation
- Lecture#1 01-14-14 Why Is Nursing of Children Different?Document12 pagesLecture#1 01-14-14 Why Is Nursing of Children Different?nkuligowskiPas encore d'évaluation
- PedsCases - Anaphylaxis Emergency TreatmentDocument5 pagesPedsCases - Anaphylaxis Emergency TreatmentSara Ilyas KhanPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar Pustakadiijah678Pas encore d'évaluation
- Ijfp 2332 287X 03 503Document4 pagesIjfp 2332 287X 03 503diijah678Pas encore d'évaluation
- Follow AupDocument6 pagesFollow Aupdiijah678Pas encore d'évaluation
- WEEKLY REPORTDocument12 pagesWEEKLY REPORTdiijah678Pas encore d'évaluation
- Sei Be Ls Eamon 2008Document9 pagesSei Be Ls Eamon 2008diijah678Pas encore d'évaluation
- Abs TrackDocument1 pageAbs Trackdiijah678Pas encore d'évaluation
- Ircmj 15 113 PDFDocument4 pagesIrcmj 15 113 PDFdiijah678Pas encore d'évaluation
- Ircmj 15 113 PDFDocument4 pagesIrcmj 15 113 PDFdiijah678Pas encore d'évaluation
- Current Management of DiverticulitisDocument51 pagesCurrent Management of Diverticulitisdiijah678Pas encore d'évaluation
- TyphoidDocument2 pagesTyphoiddiijah678Pas encore d'évaluation
- Calcium Channel Blockers For Inhibiting Preterm Labour (Review)Document31 pagesCalcium Channel Blockers For Inhibiting Preterm Labour (Review)diijah678Pas encore d'évaluation
- Pi Is 0002937810011592Document10 pagesPi Is 0002937810011592racut_khansatraPas encore d'évaluation
- A Case of Placenta Percreta With Massive Hemorrhage During Cesarean SectionDocument5 pagesA Case of Placenta Percreta With Massive Hemorrhage During Cesarean Sectiondiijah678Pas encore d'évaluation
- The Effect of Intramuscular Versus Intra-Amniotic Dexamethasone Administration On Blood Glucose Level in Diabetic Pregnant WomenDocument7 pagesThe Effect of Intramuscular Versus Intra-Amniotic Dexamethasone Administration On Blood Glucose Level in Diabetic Pregnant Womendiijah678Pas encore d'évaluation
- Pi Is 0002937810011592Document10 pagesPi Is 0002937810011592racut_khansatraPas encore d'évaluation
- Wolstenholme 2005Document11 pagesWolstenholme 2005diijah678Pas encore d'évaluation
- A Case of Placenta Percreta With Massive Hemorrhage During Cesarean SectionDocument5 pagesA Case of Placenta Percreta With Massive Hemorrhage During Cesarean Sectiondiijah678Pas encore d'évaluation
- Mekanisme Nyeri 2012Document34 pagesMekanisme Nyeri 2012Eka PutriPas encore d'évaluation
- PseudogoutDocument21 pagesPseudogoutdiijah678Pas encore d'évaluation
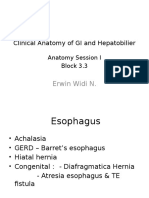
- Anatomy IDocument77 pagesAnatomy Idiijah678Pas encore d'évaluation
- Sinha Et Al-2013-Journal of NeuropsychologyDocument29 pagesSinha Et Al-2013-Journal of Neuropsychologydiijah678Pas encore d'évaluation
- Ni Hms 437509Document19 pagesNi Hms 437509diijah678Pas encore d'évaluation
- Anatomy IDocument77 pagesAnatomy Idiijah678Pas encore d'évaluation
- NVAEMQSGDocument2 pagesNVAEMQSGdiijah678Pas encore d'évaluation
- Acute Ischemic StrokeDocument206 pagesAcute Ischemic Strokediijah678Pas encore d'évaluation
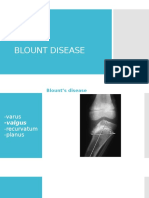
- Blount Disease1Document19 pagesBlount Disease1diijah678Pas encore d'évaluation
- Mekanisme Nyeri 2012Document34 pagesMekanisme Nyeri 2012Eka PutriPas encore d'évaluation
- Ntaios Et Al-2015-International Journal of Stroke Temperature GuidelineDocument9 pagesNtaios Et Al-2015-International Journal of Stroke Temperature Guidelinediijah678Pas encore d'évaluation
- JambanDocument21 pagesJambandiijah678Pas encore d'évaluation
- Stress PDFDocument4 pagesStress PDFYuliatyRettaHutahaeanPas encore d'évaluation
- Nephrotic Syndrome Treatment & Management - Approach Considerations, Acute NephroDocument5 pagesNephrotic Syndrome Treatment & Management - Approach Considerations, Acute NephroErvirson Jair Cañon AbrilPas encore d'évaluation
- Edwards Syndrome NotesDocument2 pagesEdwards Syndrome Notesapi-386407615Pas encore d'évaluation
- Anticoagulant, Fibrinolytic and Antiplatelet Drugs GuideDocument28 pagesAnticoagulant, Fibrinolytic and Antiplatelet Drugs GuideJagdesh SajnaniPas encore d'évaluation
- B Braun Ra - CatalogueDocument21 pagesB Braun Ra - CatalogueDina Friance ManihurukPas encore d'évaluation
- Fracture ManagementDocument58 pagesFracture Managementsaputra tri nopiantoPas encore d'évaluation
- LASIK Eye Surgery Free Consumer GuideDocument8 pagesLASIK Eye Surgery Free Consumer GuideJohn SusonPas encore d'évaluation
- Super Arrow Flex Sheath - Brochure - EN PDFDocument3 pagesSuper Arrow Flex Sheath - Brochure - EN PDFbiomedical_com_brPas encore d'évaluation
- MCQDocument6 pagesMCQalirbidiPas encore d'évaluation
- Time, Final Rinse Protocol and EndodonticsDocument1 pageTime, Final Rinse Protocol and EndodonticsvaamdevaaPas encore d'évaluation
- International Guidelines For Groin Hernia ManagementDocument165 pagesInternational Guidelines For Groin Hernia ManagementDina100% (1)
- Jcthe Role of Abutment-Attachment Selection in Resolving Inadequate Interarch Distance: A Clinical ReportdDocument7 pagesJcthe Role of Abutment-Attachment Selection in Resolving Inadequate Interarch Distance: A Clinical ReportdSyed Noorani100% (1)
- 11 Exercises For MyopiaDocument4 pages11 Exercises For MyopiaarifiqPas encore d'évaluation
- CasuitryDocument3 pagesCasuitrySoufiane ElabedPas encore d'évaluation
- Updated Resume Kelly oDocument2 pagesUpdated Resume Kelly oapi-254046653Pas encore d'évaluation
- Ventilator PortableDocument1 pageVentilator PortableAamer MumtazPas encore d'évaluation
- Diabetes - Oral KnowledgeDocument19 pagesDiabetes - Oral KnowledgeKSeegurPas encore d'évaluation
- Andre Hannah NursingresumeDocument1 pageAndre Hannah Nursingresumeapi-450112281Pas encore d'évaluation
- Or JournalDocument5 pagesOr JournalEchanique, James F.Pas encore d'évaluation
- Dall Miles Surgical ProtocolDocument16 pagesDall Miles Surgical Protocolfarnaz_2647334Pas encore d'évaluation
- Endovascular Aneurysm CoilingDocument2 pagesEndovascular Aneurysm CoilingDr. Chaim B. Colen100% (1)