Vous aimerez peut-être aussi
- Diane DaminoDocument11 pagesDiane DaminoAnup PednekarPas encore d'évaluation
- Ankle and Knee Extensor Muscle Effort During Locomotion in Young and Older Athletes: Implications For Understanding Age-Related Locomotor DeclineDocument7 pagesAnkle and Knee Extensor Muscle Effort During Locomotion in Young and Older Athletes: Implications For Understanding Age-Related Locomotor DeclineNguyễn HùngPas encore d'évaluation
- Granacheretal.2012 Gerontol CoreDocument9 pagesGranacheretal.2012 Gerontol CoreBaba DookPas encore d'évaluation
- Sullivan Et Al 2007 STEPS-CR 5Document23 pagesSullivan Et Al 2007 STEPS-CR 5Karen PohlPas encore d'évaluation
- Biomechanical Implications of Training Volume and Intensity in Aging RunnersDocument6 pagesBiomechanical Implications of Training Volume and Intensity in Aging RunnersDayana RealPas encore d'évaluation
- FIELD-FOTE, 2020 - Therapeutic Interventions To Improve Mobility With Spinal Cord Injury Related Upper Motor Neuron SyndromesDocument17 pagesFIELD-FOTE, 2020 - Therapeutic Interventions To Improve Mobility With Spinal Cord Injury Related Upper Motor Neuron SyndromesTainara Rodrigues Dos SantosPas encore d'évaluation
- Otago 1 PDFDocument3 pagesOtago 1 PDFAde Maghvira PutriPas encore d'évaluation
- Movement Analysis SummaryDocument5 pagesMovement Analysis SummaryMar diyaPas encore d'évaluation
- Damiano 2011 Comparisson Treadmill Walking CyclingDocument12 pagesDamiano 2011 Comparisson Treadmill Walking CyclingMauricio Alfredo Fuentes FloresPas encore d'évaluation
- Literature Review - Olivia MaceDocument6 pagesLiterature Review - Olivia Maceapi-499256864Pas encore d'évaluation
- Influence of Pistol Squat On Decline AngDocument10 pagesInfluence of Pistol Squat On Decline Angpedroalmeidaferro17Pas encore d'évaluation
- Strength Training for Adolescents With Cerebral Palsy (STAR)- Study Protocol of a Randomised Controlled Trial to Determine the Feasibility, Acceptability and Efficacy of Resistance Training for Adolescents With Cerebral PalsyDocument14 pagesStrength Training for Adolescents With Cerebral Palsy (STAR)- Study Protocol of a Randomised Controlled Trial to Determine the Feasibility, Acceptability and Efficacy of Resistance Training for Adolescents With Cerebral PalsyLeyla Valdebenito AlidPas encore d'évaluation
- International Journal of Health Sciences and ResearchDocument7 pagesInternational Journal of Health Sciences and ResearchRiana KhairaniPas encore d'évaluation
- Synopsis: Title-Effect of Eccentric Training and Static Stretching On Calf Muscle Tightness Among Young AdultsDocument10 pagesSynopsis: Title-Effect of Eccentric Training and Static Stretching On Calf Muscle Tightness Among Young AdultsPoonam soniPas encore d'évaluation
- Imam Subadi-Orthotic in StrokeDocument7 pagesImam Subadi-Orthotic in StrokeyudisPas encore d'évaluation
- PT Functional Training RevisitedDocument5 pagesPT Functional Training RevisitedDaniel RasiaPas encore d'évaluation
- The Back Squat Targeted Training Techniques To.2Document48 pagesThe Back Squat Targeted Training Techniques To.2Oscar Björk100% (1)
- 1 s2.0 S0966636221001338 MainDocument7 pages1 s2.0 S0966636221001338 MainLiesapriyantiPas encore d'évaluation
- Fourchet Et Al (2015) Ne Pas RetenirDocument5 pagesFourchet Et Al (2015) Ne Pas RetenirgasPas encore d'évaluation
- Agility and Perturbation TrainingDocument19 pagesAgility and Perturbation TrainingzumantaraPas encore d'évaluation
- Working With The Older Client Part 1 Article 2016Document6 pagesWorking With The Older Client Part 1 Article 2016ChrisGellertPas encore d'évaluation
- Cau Et Al. - 2014 - Center of Pressure Displacements During Gait Initiation in Individuals With ObesityDocument8 pagesCau Et Al. - 2014 - Center of Pressure Displacements During Gait Initiation in Individuals With ObesityAwatef FituriPas encore d'évaluation
- Agachamento Com Thera-Band e Ativação Dos MMI - Thera-Band Aumenta A Atividade - Foley 2017Document10 pagesAgachamento Com Thera-Band e Ativação Dos MMI - Thera-Band Aumenta A Atividade - Foley 2017AlanMeloPas encore d'évaluation
- Gait & Posture: SciencedirectDocument6 pagesGait & Posture: SciencedirectCarolina Leiva NeiraPas encore d'évaluation
- Treatment of Distal Iliotibial Band Syndrome in A Long Distance Runner With Gait Re Training Emphasizing Step Rate ManipulationDocument10 pagesTreatment of Distal Iliotibial Band Syndrome in A Long Distance Runner With Gait Re Training Emphasizing Step Rate ManipulationAlessandro ZadraPas encore d'évaluation
- 596603Document13 pages596603coachys idPas encore d'évaluation
- Treating Gait AsymmetryDocument5 pagesTreating Gait AsymmetryCherry RipePas encore d'évaluation
- Biomechanical Analysis of A BallerinaDocument4 pagesBiomechanical Analysis of A BallerinaUrooba ZubairiPas encore d'évaluation
- Lower Extremity Biomechanics During A Regular And.15Document9 pagesLower Extremity Biomechanics During A Regular And.15FaustPas encore d'évaluation
- Avoid Weight Training Plateaus & Helping Nonresponders - Based On The Teachings Of Dr. Andrew Huberman: Unlocking The Fountain Of YouthD'EverandAvoid Weight Training Plateaus & Helping Nonresponders - Based On The Teachings Of Dr. Andrew Huberman: Unlocking The Fountain Of YouthPas encore d'évaluation
- Article 2 - Current Concepts in Plyometric TrainingDocument8 pagesArticle 2 - Current Concepts in Plyometric Trainingapi-281018035Pas encore d'évaluation
- Journal MuskuloDocument15 pagesJournal Muskulotania jannahPas encore d'évaluation
- Ecor 05 0000126Document12 pagesEcor 05 0000126Lalala Safitri2000Pas encore d'évaluation
- Effect of Retro and Forward Walking On QuadricepsDocument7 pagesEffect of Retro and Forward Walking On QuadricepsRiskha Meylita PutryPas encore d'évaluation
- Jgs 12506Document8 pagesJgs 12506tpur2023Pas encore d'évaluation
- Changes in Joint Coupling and Variability During Walking Following Tibialis Posterior Muscle FatigueDocument8 pagesChanges in Joint Coupling and Variability During Walking Following Tibialis Posterior Muscle FatiguekjPas encore d'évaluation
- Core Stabilisation Training For Middleand Long-Distance RunnersDocument13 pagesCore Stabilisation Training For Middleand Long-Distance RunnersGonzalo Sebastian Bravo Rojas100% (2)
- Developing Strength and Power by Dan PfaffDocument5 pagesDeveloping Strength and Power by Dan PfaffNaija2KVeinz100% (5)
- Osteoporoz EgzersizDocument11 pagesOsteoporoz EgzersizSevtap Günay UçurumPas encore d'évaluation
- Review Article: The Effectiveness of Physical Exercise On Bone Density in Osteoporotic PatientsDocument10 pagesReview Article: The Effectiveness of Physical Exercise On Bone Density in Osteoporotic PatientsTito AlhoPas encore d'évaluation
- M. J. L. Alexander, MSC, PHD: Med Sci Sports Exerc 37:1814-1819, 2005Document2 pagesM. J. L. Alexander, MSC, PHD: Med Sci Sports Exerc 37:1814-1819, 2005stePas encore d'évaluation
- 2018 - Side Stepping With Elastics Bands and Gluteal EMGDocument11 pages2018 - Side Stepping With Elastics Bands and Gluteal EMGdiego rocioPas encore d'évaluation
- Neuromuscular Training Improves Single-Limb Stability in Young Female AthletesDocument12 pagesNeuromuscular Training Improves Single-Limb Stability in Young Female AthletesyarnlarbizimdirPas encore d'évaluation
- ACL Protocol Fowler Kennedy R Mar 2009Document21 pagesACL Protocol Fowler Kennedy R Mar 2009AleCsss123Pas encore d'évaluation
- Alterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeDocument5 pagesAlterations in Gait Velocity and Grip Strength of Stroke Survivors Following A 12-Week Structured Therapeutic Exercise ProgrammeCristina MuyargasPas encore d'évaluation
- Does Strength Training Change Your Movement Patterns?: Chris BeardsleyDocument16 pagesDoes Strength Training Change Your Movement Patterns?: Chris BeardsleyJohn Lobos100% (1)
- 5 Free Research ReviewsDocument20 pages5 Free Research ReviewsKelly AquinoPas encore d'évaluation
- Transfer of Strength and Power Training To Sports PerformanceDocument11 pagesTransfer of Strength and Power Training To Sports PerformanceEmanuel CotoPas encore d'évaluation
- Anton (2004) - Age-Related Declines in Anaerobic Muscular Performance - WL&PLDocument5 pagesAnton (2004) - Age-Related Declines in Anaerobic Muscular Performance - WL&PLJuan J. AndujarPas encore d'évaluation
- Proefschrift KlaskevankammenDocument102 pagesProefschrift Klaskevankammenxian karachiPas encore d'évaluation
- Materi PIR - Dr. S M Mei Wulan, SP - KFR-K Application of Movement - Therapeutic Exercise in Cerebral PalsyDocument26 pagesMateri PIR - Dr. S M Mei Wulan, SP - KFR-K Application of Movement - Therapeutic Exercise in Cerebral PalsyGhea Putri HendrianiPas encore d'évaluation
- Orthotic Management of Children With Cerebral PalsyDocument9 pagesOrthotic Management of Children With Cerebral PalsyEslam ElsayedPas encore d'évaluation
- Bioengineering 09 00272Document13 pagesBioengineering 09 00272Jordi Cortizo MoleraPas encore d'évaluation
- Glut MedMaxDocument12 pagesGlut MedMaxColm CoakleyPas encore d'évaluation
- The Infuence of Running On Lower Limb Cartilage - A Systematic Review and Meta AnalysisDocument20 pagesThe Infuence of Running On Lower Limb Cartilage - A Systematic Review and Meta Analysismonalisa.fiscalPas encore d'évaluation
- 79b6 PDFDocument5 pages79b6 PDFcnsatishPas encore d'évaluation
- Chaos Agility Training 2009Document36 pagesChaos Agility Training 2009ok okPas encore d'évaluation
- Functional Training for Athletes at All Levels: Workouts for Agility, Speed and PowerD'EverandFunctional Training for Athletes at All Levels: Workouts for Agility, Speed and PowerÉvaluation : 4 sur 5 étoiles4/5 (2)
- Dynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionD'EverandDynamic Stretching: The Revolutionary New Warm-up Method to Improve Power, Performance and Range of MotionÉvaluation : 5 sur 5 étoiles5/5 (1)
- FallsintheElderly PDFDocument12 pagesFallsintheElderly PDFNa d'Nazaie CodePas encore d'évaluation
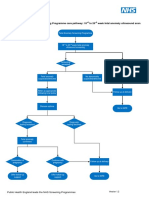
- FASPDownsT21EdwardsT18andPatausT13pathway11 PDFDocument1 pageFASPDownsT21EdwardsT18andPatausT13pathway11 PDFNa d'Nazaie CodePas encore d'évaluation
- 2 10 1 PBDocument3 pages2 10 1 PBNa d'Nazaie CodePas encore d'évaluation
- FallsintheElderly PDFDocument12 pagesFallsintheElderly PDFNa d'Nazaie CodePas encore d'évaluation
- Enhancing Nurses Pain Assessment To Improve.11Document2 pagesEnhancing Nurses Pain Assessment To Improve.11Na d'Nazaie CodePas encore d'évaluation
- Model Klasifikasi Menggunakan Metode Regresi Logistik Dan Multivariate Adaptive Regression Splines (Mars) (Studi Kasus: Data Survei Biaya Hidup (SBH) Kota Kediri Tahun 2012)Document12 pagesModel Klasifikasi Menggunakan Metode Regresi Logistik Dan Multivariate Adaptive Regression Splines (Mars) (Studi Kasus: Data Survei Biaya Hidup (SBH) Kota Kediri Tahun 2012)Na d'Nazaie CodePas encore d'évaluation
- FASP Fetal Anomaly Ultrasound Screening Pathwayv12Document1 pageFASP Fetal Anomaly Ultrasound Screening Pathwayv12Na d'Nazaie CodePas encore d'évaluation
- Rita Dwi HartantiDocument9 pagesRita Dwi HartantiNa d'Nazaie CodePas encore d'évaluation
- Kusiima Chs Masters Abstract PDFDocument3 pagesKusiima Chs Masters Abstract PDFNa d'Nazaie CodePas encore d'évaluation
- Kualitas HidupDocument8 pagesKualitas Hidupsrihandayani1984Pas encore d'évaluation
- ITS Undergraduate 18940 Bibliographypdf PDFDocument2 pagesITS Undergraduate 18940 Bibliographypdf PDFNa d'Nazaie CodePas encore d'évaluation
- TB Riskfactors SocialdeterminantsDocument7 pagesTB Riskfactors SocialdeterminantsNa d'Nazaie CodePas encore d'évaluation
- R1 - Vo3No4 KJHDocument14 pagesR1 - Vo3No4 KJHNa d'Nazaie CodePas encore d'évaluation
- Ipi200729 PDFDocument14 pagesIpi200729 PDFNa d'Nazaie CodePas encore d'évaluation
- Calculating The Sample Size of Multivariate Populations: Norms of RepresentationDocument6 pagesCalculating The Sample Size of Multivariate Populations: Norms of RepresentationNa d'Nazaie CodePas encore d'évaluation
- WOQOL Measuring QV MentalDocument15 pagesWOQOL Measuring QV MentalpenfoPas encore d'évaluation
- McCallum (2001) Sample Size in Factor Analysis The Role of Model ErrorDocument27 pagesMcCallum (2001) Sample Size in Factor Analysis The Role of Model ErrorNa d'Nazaie CodePas encore d'évaluation
- Dochtermann Jenkins ResponseDocument11 pagesDochtermann Jenkins ResponseNa d'Nazaie CodePas encore d'évaluation
- Circulation 2014 Hansen 1859 67Document15 pagesCirculation 2014 Hansen 1859 67Na d'Nazaie CodePas encore d'évaluation
- JurnalDocument87 pagesJurnalNa d'Nazaie CodePas encore d'évaluation
- Power and Minimal Sample Size For Multivariate Analysis of MicroarraysDocument1 pagePower and Minimal Sample Size For Multivariate Analysis of MicroarraysNa d'Nazaie CodePas encore d'évaluation
- 20Document3 pages20Na d'Nazaie CodePas encore d'évaluation
- Circulation 2014 Hansen 1859 67Document15 pagesCirculation 2014 Hansen 1859 67Na d'Nazaie CodePas encore d'évaluation
- Kuesioner SSQDocument15 pagesKuesioner SSQNa d'Nazaie Code100% (3)
- Toxicon: SciencedirectDocument14 pagesToxicon: SciencedirectNa d'Nazaie CodePas encore d'évaluation
- The Blind MotherDocument2 pagesThe Blind MotherNa d'Nazaie CodePas encore d'évaluation
- 995 FullDocument8 pages995 FullNa d'Nazaie CodePas encore d'évaluation
- Circulation 2011 Kilgannon 2717 22Document7 pagesCirculation 2011 Kilgannon 2717 22Na d'Nazaie CodePas encore d'évaluation
- Week 1 Week 2 Week 3 Week 4 Week 5: Xmil ChallengeDocument2 pagesWeek 1 Week 2 Week 3 Week 4 Week 5: Xmil ChallengeJorge MamaguevPas encore d'évaluation
- Principles Behind The Exercise-Based Physical ActivitiesDocument10 pagesPrinciples Behind The Exercise-Based Physical ActivitiesJen TeruelPas encore d'évaluation
- Wendler 531 - BLANKDocument10 pagesWendler 531 - BLANKJenny LePas encore d'évaluation
- Dinamik StretchingDocument38 pagesDinamik StretchingLing Lii Lik100% (2)
- Kizen 16 Week PowerbuildingDocument16 pagesKizen 16 Week PowerbuildingDamien SeowPas encore d'évaluation
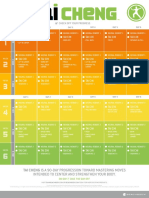
- Tai ChenDocument2 pagesTai ChenjaviPas encore d'évaluation
- CFK Trainer CourseDocument163 pagesCFK Trainer CoursezumadumaPas encore d'évaluation
- H.O.P.E 3 Module 1 (Jenny Mae D. Otto Grade 12 Abm-Yen)Document8 pagesH.O.P.E 3 Module 1 (Jenny Mae D. Otto Grade 12 Abm-Yen)Jenny Mae OttoPas encore d'évaluation
- 50 Life Secrets and TipsDocument10 pages50 Life Secrets and TipsDarkPoolPas encore d'évaluation
- 100 Tabata Workouts PDFDocument33 pages100 Tabata Workouts PDFharris81Pas encore d'évaluation
- SAMPLE 2 - Writing An ArticleDocument2 pagesSAMPLE 2 - Writing An ArticleMiz MalinzPas encore d'évaluation
- S. Shaw WorkoutsDocument11 pagesS. Shaw WorkoutsMarcePas encore d'évaluation
- TRACK AND FIELD 2015 Training PlanDocument8 pagesTRACK AND FIELD 2015 Training PlanHazwan StyntethPas encore d'évaluation
- PEDH 112 Fourth Quarter ExamDocument4 pagesPEDH 112 Fourth Quarter ExamJoshua Azura0% (1)
- 30 Sentence in TiniklingDocument1 page30 Sentence in Tinikling1 Callejo Jr, michael B.Pas encore d'évaluation
- Freeletics Cardio & Strength Guide IIDocument1 pageFreeletics Cardio & Strength Guide IIElena SavaPas encore d'évaluation
- Shredding IntermediateDocument66 pagesShredding IntermediateAbdulaziz Abumelha100% (1)
- Free Chakra Posters Gift - Karma Gaia (2) - CompressedDocument9 pagesFree Chakra Posters Gift - Karma Gaia (2) - Compressed4lm402100% (1)
- Core Crusher Hannah EdenDocument11 pagesCore Crusher Hannah Edenalaa bachacha67% (3)
- Prelim-P E1Document2 pagesPrelim-P E1jpenagunda23Pas encore d'évaluation
- Dhirendra Brahmachari - Yogasana VijnanaDocument390 pagesDhirendra Brahmachari - Yogasana VijnanaKulin ShahPas encore d'évaluation
- PRmaa 20160517 TingcangADocument6 pagesPRmaa 20160517 TingcangAMary May AbellonPas encore d'évaluation
- 12 Week Free Bodybuilding Program Part 1Document4 pages12 Week Free Bodybuilding Program Part 1secondtexanPas encore d'évaluation
- AmarulaDocument1 pageAmarulaEdwardPas encore d'évaluation
- 7-Day Bootcamp Workout Plan: Get Results With These Variety-Packed WorkoutsDocument2 pages7-Day Bootcamp Workout Plan: Get Results With These Variety-Packed WorkoutskenbocbrPas encore d'évaluation
- Programme Gratuit Full Body Push Pull Leg Upper Lower We Gonna Make ItDocument240 pagesProgramme Gratuit Full Body Push Pull Leg Upper Lower We Gonna Make Itsarin44473Pas encore d'évaluation
- Learning Motor Skills Golf ExampleDocument5 pagesLearning Motor Skills Golf ExamplesdjuknicPas encore d'évaluation
- Active Program HastingsDocument25 pagesActive Program HastingsrosaPas encore d'évaluation
- Old School Iron Month 1Document9 pagesOld School Iron Month 14wkbyp8bt5Pas encore d'évaluation
- MiCoach Zone User ManualDocument15 pagesMiCoach Zone User ManualJose A. FlorPas encore d'évaluation