Vous aimerez peut-être aussi
- Obrazovanje Temeljeno Na SnagamaDocument19 pagesObrazovanje Temeljeno Na SnagamaNeven BuhinPas encore d'évaluation
- Correct Spherical Errors with Subjective RefractionDocument11 pagesCorrect Spherical Errors with Subjective RefractionMagfirah HalimPas encore d'évaluation
- Does Pain Behavior Infl UenceDocument4 pagesDoes Pain Behavior Infl UenceNeven BuhinPas encore d'évaluation
- Knowldege & Attitude Survey 7-14Document10 pagesKnowldege & Attitude Survey 7-14Princess Kathleen Bascos LagunaPas encore d'évaluation
- Chronic Pain in ChildrenDocument9 pagesChronic Pain in ChildrenNeven BuhinPas encore d'évaluation
- History NursingDocument20 pagesHistory NursingNeven BuhinPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5783)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Mental Health & TravelDocument18 pagesMental Health & TravelReyza HasnyPas encore d'évaluation
- South Autralia RMO Application GuideDocument35 pagesSouth Autralia RMO Application GuideSOMANATHAN UMAHSUTHANPas encore d'évaluation
- BrochureDocument20 pagesBrochureAnjali MohanPas encore d'évaluation
- Workload Indicator of Staffing Need - WiSN - IndonesiaDocument11 pagesWorkload Indicator of Staffing Need - WiSN - IndonesiaPardjono KromoredjoPas encore d'évaluation
- Kenya ARV Guidelines 2018Document230 pagesKenya ARV Guidelines 2018Felix Wafula MusibiPas encore d'évaluation
- Practice Nurse Vacancy Oct 2019Document2 pagesPractice Nurse Vacancy Oct 2019M LubisPas encore d'évaluation
- QADM in Health Care IndustryDocument12 pagesQADM in Health Care IndustryYogesh WaghPas encore d'évaluation
- The Burma Code Vol-4Document438 pagesThe Burma Code Vol-4kerrypwlPas encore d'évaluation
- DQSP-00033 Storage and shipmentDocument13 pagesDQSP-00033 Storage and shipmentalexvo.1612Pas encore d'évaluation
- Pathway PDFDocument4 pagesPathway PDFSunny RatnaniPas encore d'évaluation
- Crvreport PDFDocument1 pageCrvreport PDFمرتجز حیدرPas encore d'évaluation
- AMSA Code of EthicsDocument4 pagesAMSA Code of EthicsChristian KwokPas encore d'évaluation
- Calories Needed For A 19 Year Old, 81 KG MaleDocument1 pageCalories Needed For A 19 Year Old, 81 KG MaleDoaa DodeyPas encore d'évaluation
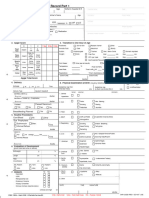
- Form1583A NewbornRecord1and2Document4 pagesForm1583A NewbornRecord1and2miguealliPas encore d'évaluation
- Pharmacy Profession in Nepal Has History Only of About 50 Years BackDocument4 pagesPharmacy Profession in Nepal Has History Only of About 50 Years BackSushant Aryal100% (1)
- M50ADocument44 pagesM50AHassab SaeedPas encore d'évaluation
- Fundamentals of Patient SafetyDocument2 pagesFundamentals of Patient SafetySarah AjodhaPas encore d'évaluation
- Skin Infection Around A Fingernail or Toenail (Paronychia)Document3 pagesSkin Infection Around A Fingernail or Toenail (Paronychia)Ortopedia HGMPas encore d'évaluation
- Staffing&SchedulingDocument14 pagesStaffing&SchedulingKrishnaveni MurugeshPas encore d'évaluation
- Standards and Guidelines For Electronic Medical Record Systems in KenyaDocument115 pagesStandards and Guidelines For Electronic Medical Record Systems in KenyaI-TECH KenyaPas encore d'évaluation
- Healthcare FinancingDocument15 pagesHealthcare FinancingMOZAIDPas encore d'évaluation
- Comfort Dental Fee-Schedule-MO-KS-2014-accessibleDocument1 pageComfort Dental Fee-Schedule-MO-KS-2014-accessibleAllen WilburPas encore d'évaluation
- Epidemiology of Adult Rheumatoid Arthritis: Yannis Alamanos, Alexandros A. DrososDocument7 pagesEpidemiology of Adult Rheumatoid Arthritis: Yannis Alamanos, Alexandros A. DrososAkmal FachriansyahPas encore d'évaluation
- Kierstens Resume and References-2Document2 pagesKierstens Resume and References-2api-394845409Pas encore d'évaluation
- Biomedicalwastemanagement 180429140745Document39 pagesBiomedicalwastemanagement 180429140745SSR PRASAD KOVELAMUDIPas encore d'évaluation
- W W W W W: ABC and VED Analysis in Medical Stores Inventory ControlDocument3 pagesW W W W W: ABC and VED Analysis in Medical Stores Inventory ControlRaviraj KamblePas encore d'évaluation
- Literature Review On Leadership in Healthcare Management: ISSN 2329-9150 2018, Vol. 5, No. 1Document10 pagesLiterature Review On Leadership in Healthcare Management: ISSN 2329-9150 2018, Vol. 5, No. 1cirilaPas encore d'évaluation
- Remedial Test in Mapeh 10Document2 pagesRemedial Test in Mapeh 10Reu Well50% (2)
- Khoury 2013 Mindfulness-Metaanalys PDFDocument9 pagesKhoury 2013 Mindfulness-Metaanalys PDFImanol MendizabalPas encore d'évaluation
- Announcement For Postgraduate Programmes 2024 2025 1Document12 pagesAnnouncement For Postgraduate Programmes 2024 2025 1fredrick damianPas encore d'évaluation