Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Cervical DystociaDocument22 pagesCervical DystociaBaldau TiwariPas encore d'évaluation
- Feline Anemia Diagnostic AlgorithmDocument1 pageFeline Anemia Diagnostic AlgorithmEd BlackadderPas encore d'évaluation
- FNCP - Inadequate Exercise & Breeding Site For MosquitoesDocument2 pagesFNCP - Inadequate Exercise & Breeding Site For MosquitoesGwyneth Fisher100% (1)
- Crohn Vs ColitisDocument5 pagesCrohn Vs Colitiswbarnes7Pas encore d'évaluation
- Notes by Dr. Khurram PDFDocument22 pagesNotes by Dr. Khurram PDFAdnan AsgharPas encore d'évaluation
- Severe Ulcerative Colitis UHL Childrens Medical GuidelineDocument8 pagesSevere Ulcerative Colitis UHL Childrens Medical GuidelineFanny PritaningrumPas encore d'évaluation
- High Voltage Galvanic Current Lecture PDFDocument22 pagesHigh Voltage Galvanic Current Lecture PDFdespPas encore d'évaluation
- Cardiogenic SyokDocument51 pagesCardiogenic SyokRamadhyanPas encore d'évaluation
- All India Ayush Post Graduate Entrance Test 2019 Question PaperDocument24 pagesAll India Ayush Post Graduate Entrance Test 2019 Question PaperSoumitra BosePas encore d'évaluation
- Kode DiagnosaDocument6 pagesKode DiagnosaRoy SuhendraPas encore d'évaluation
- Progeria Case StudyDocument12 pagesProgeria Case StudyChristein Roger Dondoyano GamalePas encore d'évaluation
- Hypoglycemia in Adults Clinical Manifestations, Definition, and CausesDocument1 pageHypoglycemia in Adults Clinical Manifestations, Definition, and CausesnovaPas encore d'évaluation
- Peace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Document4 pagesPeace Corps Vaccine Administration Schedule - TG 300 Medical Technical Guideline 300 - July 2008Accessible Journal Media: Peace Corps Documents100% (1)
- Identifikasi Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Pandai BesiDocument10 pagesIdentifikasi Risiko Musculoskeletal Disorders (MSDS) Pada Pekerja Pandai BesiTito MuharamPas encore d'évaluation
- Case PresentationDocument11 pagesCase PresentationHira Rafique100% (1)
- Acute AbdomenDocument31 pagesAcute AbdomenWildan AngelouPas encore d'évaluation
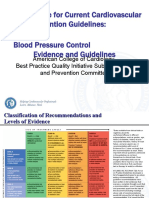
- 3 ACC Prevention Blood PressureDocument69 pages3 ACC Prevention Blood PressureMelissa Delgado100% (1)
- L17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikDocument75 pagesL17. Askep Kritis Dan Gadar Pasien Dengan Ggguan Sistem Pernafan NontraumatikSepto KristianaPas encore d'évaluation
- Hamdard Fehrist-e-Advia PDFDocument109 pagesHamdard Fehrist-e-Advia PDFdvtherion100% (1)
- Shutter Island Presentation For ArtifactDocument8 pagesShutter Island Presentation For Artifactapi-478108843Pas encore d'évaluation
- Virulence Factors of Streptococcus PyogenesDocument6 pagesVirulence Factors of Streptococcus PyogenesAmador GielasPas encore d'évaluation
- UCDocument6 pagesUCapiv2010_808955526Pas encore d'évaluation
- TP3 Ingles II 19Document3 pagesTP3 Ingles II 19Gustavo ArenaPas encore d'évaluation
- Artikel Bahan Ujian PraktikumDocument10 pagesArtikel Bahan Ujian PraktikumTakiaGenjiPas encore d'évaluation
- Dengue Fever: A Statistical Analysis Regarding Awareness About Dengue Among University Students in Azad KashmirDocument8 pagesDengue Fever: A Statistical Analysis Regarding Awareness About Dengue Among University Students in Azad KashmirIm jungkook JUSTIN SEAGULL A.K.A jungshookPas encore d'évaluation
- DR - Thompsons CBC-RBC Indices Guide - A Guide To Red Blood Cell IndicesDocument54 pagesDR - Thompsons CBC-RBC Indices Guide - A Guide To Red Blood Cell IndicesYohana SetiawanPas encore d'évaluation
- Specimen Rejection Criteria - The Doctors LaboratoryDocument2 pagesSpecimen Rejection Criteria - The Doctors LaboratoryRevathyPas encore d'évaluation
- PRECIO PromalabDocument6 pagesPRECIO PromalabJenny QuingaPas encore d'évaluation
- DKA CME 23.08.2023 Edited FinalleDocument20 pagesDKA CME 23.08.2023 Edited FinalleDeborah ChemutaiPas encore d'évaluation
- JournalDocument6 pagesJournalIka RachmadantPas encore d'évaluation