Vous aimerez peut-être aussi
- Colon Cancer Pathophysiology PDFDocument2 pagesColon Cancer Pathophysiology PDFMaggiePas encore d'évaluation
- The Original Prevention of Sickness PamphletDocument88 pagesThe Original Prevention of Sickness PamphletGeorge Singleton100% (4)
- ResearchDocument26 pagesResearchJhen de Vera83% (12)
- JCO 2003 Lin 631 7Document7 pagesJCO 2003 Lin 631 7Adhika Manggala DharmaPas encore d'évaluation
- Prognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentDocument7 pagesPrognostic Factors in Nasopharyngeal Carcinoma With Synchronous Liver Metastasis: A Retrospective Study For The Management of TreatmentChairul Nurdin AzaliPas encore d'évaluation
- (583950958) Journal Leucopenia Treatment Effiicacy NPCDocument8 pages(583950958) Journal Leucopenia Treatment Effiicacy NPCDaniel HoseaPas encore d'évaluation
- ProtocolsummaryDocument3 pagesProtocolsummaryapi-644802109Pas encore d'évaluation
- Lung Stereotactic Ablative Body Radiotheray SABR - Patient o - 2019 - ClinicalDocument1 pageLung Stereotactic Ablative Body Radiotheray SABR - Patient o - 2019 - ClinicalSEPas encore d'évaluation
- Prognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated RadiotherapyDocument7 pagesPrognostic Model For Survival of Local Recurrent Nasopharyngeal Carcinoma With Intensity-Modulated Radiotherapypp kabsemarangPas encore d'évaluation
- Annotated BibDocument16 pagesAnnotated Bibapi-542958465Pas encore d'évaluation
- Jurnal CNFDocument36 pagesJurnal CNFAndrianorMuhammadPas encore d'évaluation
- 3781 FullDocument6 pages3781 FullSukhvinder Singh RanaPas encore d'évaluation
- 10.12921 cmst.2006.12.02.143-147 MoczkoDocument5 pages10.12921 cmst.2006.12.02.143-147 Moczkoshital shermalePas encore d'évaluation
- 1 s2.0 S0923753419363677 MainDocument6 pages1 s2.0 S0923753419363677 MainSamantha AdriannePas encore d'évaluation
- Background: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckDocument10 pagesBackground: Nivolumab For Recurrent Squamous-Cell Carcinoma of The Head and NeckjoitPas encore d'évaluation
- Concurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung CancerDocument7 pagesConcurrent Cisplatin, Etoposide, and Chest Radiotherapy in Pathologic Stage IIIB Non-Small-Cell Lung Cancerdurgesh kumarPas encore d'évaluation
- Ou 2016Document8 pagesOu 2016tami widiatul azahraPas encore d'évaluation
- Clinical StudyDocument7 pagesClinical StudyTit fuckerPas encore d'évaluation
- NPCDocument8 pagesNPCArsy Mira PertiwiPas encore d'évaluation
- 33Document11 pages33Joana KellenPas encore d'évaluation
- 551 PDFDocument5 pages551 PDFfaidgustisyarifPas encore d'évaluation
- 9 - RiDocument1 page9 - RisiuroPas encore d'évaluation
- Cancer of The EsophagusDocument6 pagesCancer of The EsophagusDileep SrinivasanPas encore d'évaluation
- MeduloblastomaDocument7 pagesMeduloblastomasilvia erfanPas encore d'évaluation
- CapeOX ChronicleDocument22 pagesCapeOX ChronicleOttofianus Hewick KalangiPas encore d'évaluation
- 4451 FullDocument4 pages4451 FullSukhvinder Singh RanaPas encore d'évaluation
- Concurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaDocument5 pagesConcurrent Radiotherapy and Weekly Paclitaxel For Locally Advanced Squmous Cell Carcinoma of Uterine Cervix-Treated Patients at Rural Centre in IndiaIjsrnet EditorialPas encore d'évaluation
- Background: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyDocument11 pagesBackground: Concurrent Chemoradiotherapy (CRT) Is The: Correspondence To: DR A.S.C. Wong, Department of HematologyJordan SantosPas encore d'évaluation
- Clinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDocument7 pagesClinico-Radiological Co-Relation of Carcinoma Larynx and Hypopharynx: A Prospective StudyDede MarizalPas encore d'évaluation
- Hyerbaric Oxygenation - Final DraftDocument17 pagesHyerbaric Oxygenation - Final Draftapi-542958465Pas encore d'évaluation
- Erbitux MonotherapyDocument7 pagesErbitux MonotherapyMaulik PatelPas encore d'évaluation
- GP 96Document24 pagesGP 96Study MaterialPas encore d'évaluation
- Journal of Clinical Oncology Volume 32 Number 19 July 2014Document10 pagesJournal of Clinical Oncology Volume 32 Number 19 July 2014ivssonPas encore d'évaluation
- TNBC PMRTDocument7 pagesTNBC PMRTMed MedPas encore d'évaluation
- BJC 2013230Document6 pagesBJC 2013230Abraham OsunaPas encore d'évaluation
- Clinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypeDocument12 pagesClinical Impact of External Radiotherapy in Non-Metastatic Esophageal Cancer According To Histopathological SubtypesilviailiePas encore d'évaluation
- Moretto 2014Document8 pagesMoretto 2014Silvie WidyaPas encore d'évaluation
- Head NeckDocument8 pagesHead NeckerandolphsavagePas encore d'évaluation
- Capecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal CancerDocument6 pagesCapecitabine Monotherapy For Recurrent and Metastatic Nasopharyngeal Cancertrifamonika23Pas encore d'évaluation
- Prediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataDocument10 pagesPrediction Model For Shortterm Mortality After Palliative Therapy For Patients Having Advanced Cancer - A Cohort Study From Routine Electronic Medical DataHollis LukPas encore d'évaluation
- EBRT in DTCDocument7 pagesEBRT in DTCElena FlorentinaPas encore d'évaluation
- Chua 2005 Long-Term Survival After Cisplatin-Based InductionDocument7 pagesChua 2005 Long-Term Survival After Cisplatin-Based InductionFitria WaffiPas encore d'évaluation
- Faen ZhangDocument6 pagesFaen ZhangAlejandro TurnerPas encore d'évaluation
- Primary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyDocument7 pagesPrimary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyLuvita Amallia SyadhatinPas encore d'évaluation
- IAEA HPFX 2015Document6 pagesIAEA HPFX 2015Johana PatiñoPas encore d'évaluation
- Intergroup 0123Document8 pagesIntergroup 0123radonc17Pas encore d'évaluation
- Sequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomaDocument9 pagesSequential Chemoradiotherapy With Gemcitabine and Cisplatin For Locoregionally Advanced Nasopharyngeal CarcinomadheaonyonPas encore d'évaluation
- Portec 2.Document8 pagesPortec 2.henryPas encore d'évaluation
- 2020 Central Airway Toxicity After High Dose Radiation - A Combined Analysis of Prospective Clinical Trials For NSCLCDocument25 pages2020 Central Airway Toxicity After High Dose Radiation - A Combined Analysis of Prospective Clinical Trials For NSCLCromaana3540Pas encore d'évaluation
- 2018 Article 6554Document8 pages2018 Article 6554Raíla SoaresPas encore d'évaluation
- Se Hacía Biopsia A Los Tres Meses. Estudio Pequeño ADocument5 pagesSe Hacía Biopsia A Los Tres Meses. Estudio Pequeño Aouf81Pas encore d'évaluation
- ReferensiDocument7 pagesReferensireza amahoruPas encore d'évaluation
- P. Wang Et Al.2019Document6 pagesP. Wang Et Al.2019Mai M. AlshalPas encore d'évaluation
- Bisa 1Document8 pagesBisa 1justforuroPas encore d'évaluation
- Recent Advances With Topotecan in The Treatment of Lung CancerDocument13 pagesRecent Advances With Topotecan in The Treatment of Lung Cancerapi-3821924Pas encore d'évaluation
- Neoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesDocument6 pagesNeoadjuvant Paclitaxel For Operable Breast Cancer: Multicenter Phase II Trial With Clinical OutcomesSubhash SugathanPas encore d'évaluation
- Prophylactic Cervical Lymph Node Irradiation Provides No Benefit For Patients of Stage IE Extranodal Natural Killer/t Cell Lymphoma, Nasal TypeDocument8 pagesProphylactic Cervical Lymph Node Irradiation Provides No Benefit For Patients of Stage IE Extranodal Natural Killer/t Cell Lymphoma, Nasal TypeCleysser Antonio Custodio PolarPas encore d'évaluation
- 1677 5538 Ibju 42 04 0694Document10 pages1677 5538 Ibju 42 04 0694Lucas VibiamPas encore d'évaluation
- ARTSCANIIIDocument61 pagesARTSCANIIIKishoreChandraKoradaPas encore d'évaluation
- SouthAsianJCancer6115-2517942 065939Document5 pagesSouthAsianJCancer6115-2517942 065939Gibi SupitPas encore d'évaluation
- Intensity-Modulated or Conformal Radiotherapy Improves The Quality of Life of Patients With Nasopharyngeal CarcinomaDocument10 pagesIntensity-Modulated or Conformal Radiotherapy Improves The Quality of Life of Patients With Nasopharyngeal CarcinomaAde Febrian RamadhanPas encore d'évaluation
- Carsinoma NasopharyngealDocument9 pagesCarsinoma NasopharyngealRahma R SPas encore d'évaluation
- Radiotherapy of Liver CancerD'EverandRadiotherapy of Liver CancerJinsil SeongPas encore d'évaluation
- Jurnal KIEDocument6 pagesJurnal KIEdenanurbaniazharPas encore d'évaluation
- Care Planning FarmasiDocument87 pagesCare Planning FarmasiYayaPas encore d'évaluation
- Jurnal Analisis Biaya (BEP) (Sainstech, Volume 22, Nomor 1, Januari 2012)Document12 pagesJurnal Analisis Biaya (BEP) (Sainstech, Volume 22, Nomor 1, Januari 2012)denanurbaniazharPas encore d'évaluation
- Aplikasi Rehabilitasi Berhenti Merokok: 1 PendahuluanDocument6 pagesAplikasi Rehabilitasi Berhenti Merokok: 1 PendahuluandenanurbaniazharPas encore d'évaluation
- 10.1016j.amjcard.2010.01.355 FurosemidDocument4 pages10.1016j.amjcard.2010.01.355 FurosemiddenanurbaniazharPas encore d'évaluation
- Intravenous Paracetamol: Safe Anaesthesia Liaison GroupDocument3 pagesIntravenous Paracetamol: Safe Anaesthesia Liaison GroupdenanurbaniazharPas encore d'évaluation
- AlbuminDocument5 pagesAlbumindenanurbaniazharPas encore d'évaluation
- Chan 2014Document7 pagesChan 2014denanurbaniazharPas encore d'évaluation
- Qian-Sheng Ke, M.D., Hann-Chorng Kuo, M.DDocument4 pagesQian-Sheng Ke, M.D., Hann-Chorng Kuo, M.DdenanurbaniazharPas encore d'évaluation
- Assessment of Chest Pain in Primary CareDocument8 pagesAssessment of Chest Pain in Primary CareVictoria GomezPas encore d'évaluation
- Latihan 6 KSPT - Dian Kusuma Atmaja - 19104023Document2 pagesLatihan 6 KSPT - Dian Kusuma Atmaja - 19104023Tia NingPas encore d'évaluation
- Medical Surgical Nursing Nclex QuestionsDocument82 pagesMedical Surgical Nursing Nclex Questionsdee_day_893% (14)
- Phlebotomy Handbook: Blood Collection EssentialsDocument55 pagesPhlebotomy Handbook: Blood Collection EssentialsayooniaPas encore d'évaluation
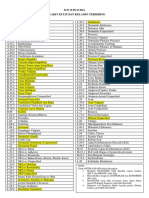
- Icd 10 Inacbgs Penyakit Kulit Dan Kelamin TerseringDocument1 pageIcd 10 Inacbgs Penyakit Kulit Dan Kelamin TerseringCempaka limaPas encore d'évaluation
- It's Official! Vegetarian Centenarians Are Happier Healthier Than Aging Meat-eaters - Mrs. Nasib Kaur Surpasses 100 Years Old Eating Plant-based Diet and Loving It - Majid Ali, Nir Barzilai - Non-LowCarb Non-Paleo Longevity DietDocument3 pagesIt's Official! Vegetarian Centenarians Are Happier Healthier Than Aging Meat-eaters - Mrs. Nasib Kaur Surpasses 100 Years Old Eating Plant-based Diet and Loving It - Majid Ali, Nir Barzilai - Non-LowCarb Non-Paleo Longevity DietPaleoCentenarianDietPas encore d'évaluation
- Histopathology Requisition FormDocument2 pagesHistopathology Requisition Formr4rahePas encore d'évaluation
- UrinalysisDocument36 pagesUrinalysisMarl EstradaPas encore d'évaluation
- Formalin MsdsDocument7 pagesFormalin MsdsSalsabilaAzisPas encore d'évaluation
- Symptom Distress Scale User ManualDocument99 pagesSymptom Distress Scale User ManualLivianty HukubunPas encore d'évaluation
- Article 1Document4 pagesArticle 1Tashu SardaPas encore d'évaluation
- Diabetic Microvascular DiseaseDocument68 pagesDiabetic Microvascular DiseasePavel GonzálezPas encore d'évaluation
- Palliative Bilio Digestive Anastomosis For The Treatment of Bile Duct Obstruction Due To Pancreatic Head Tumors Techniques and Therapeutic ResultsDocument10 pagesPalliative Bilio Digestive Anastomosis For The Treatment of Bile Duct Obstruction Due To Pancreatic Head Tumors Techniques and Therapeutic ResultsAthenaeum Scientific PublishersPas encore d'évaluation
- The Management of Diarrhoea in Adults: RCN Guidance For Nursing StaffDocument35 pagesThe Management of Diarrhoea in Adults: RCN Guidance For Nursing StaffPopa ElenaPas encore d'évaluation
- QUILICOTDocument5 pagesQUILICOTJoshua ParilPas encore d'évaluation
- GRP2Document87 pagesGRP2Veronica ChanPas encore d'évaluation
- Physical Assessment - IntegumentDocument102 pagesPhysical Assessment - IntegumentDeeeeePas encore d'évaluation
- Chapman's Reflexes and Modern Clinical Applications - Lecture - William H. Devine, DODocument94 pagesChapman's Reflexes and Modern Clinical Applications - Lecture - William H. Devine, DOHermann92% (12)
- Tanta Neuro MCQDocument9 pagesTanta Neuro MCQBadr Diham100% (1)
- Clinical Methods in ENT by P. T. WakodeDocument229 pagesClinical Methods in ENT by P. T. WakodeQuranSunnat100% (1)
- Malunggay MonographDocument9 pagesMalunggay Monographkiara4decenaPas encore d'évaluation
- Rubrics For Children in MurphyDocument18 pagesRubrics For Children in MurphyVirag PatilPas encore d'évaluation
- Informative Speech 1Document3 pagesInformative Speech 1Janiela MariePas encore d'évaluation
- VALERIAN Fact SheetDocument13 pagesVALERIAN Fact SheetNZHHPas encore d'évaluation
- Myelopathy: Dr. Astra Dea Simanungkalit, SpsDocument24 pagesMyelopathy: Dr. Astra Dea Simanungkalit, SpspppkkkPas encore d'évaluation
- CA Oral CavityDocument53 pagesCA Oral Cavityaakash11Pas encore d'évaluation