Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Jadwal Jaga IGD 1Document25 pagesJadwal Jaga IGD 1retPas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Itinerary BALIDocument7 pagesItinerary BALIretPas encore d'évaluation
- Daftar Kelulusan Osce November 2018 PDFDocument73 pagesDaftar Kelulusan Osce November 2018 PDFAisyah Althafunnisa Bayu PutriPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- EaasmcDocument27 pagesEaasmcretPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Ante Natal CareDocument82 pagesAnte Natal CareretPas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Group Moderators' Manual BookDocument37 pagesGroup Moderators' Manual BookretPas encore d'évaluation
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- New Text DocumentDocument1 pageNew Text DocumentretPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Soy Milk Consumption and Blood Pressure Among Type 2 Diabetic Patients With NephropathyDocument7 pagesSoy Milk Consumption and Blood Pressure Among Type 2 Diabetic Patients With NephropathyretPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A B C D E: Senin Selasa Rabu Kamis Jumat SabtuDocument11 pagesA B C D E: Senin Selasa Rabu Kamis Jumat SabturetPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- New Text DocumentDocument1 pageNew Text DocumentretPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grafik GDS Ny. I: Tanggal PemeriksaanDocument7 pagesGrafik GDS Ny. I: Tanggal PemeriksaanretPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- 4-Planning Tools & TechniquesDocument17 pages4-Planning Tools & TechniquesretPas encore d'évaluation
- Bali Corat CoretDocument1 pageBali Corat CoretretPas encore d'évaluation
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Meeting 3Document28 pagesMeeting 3retPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Countries' Etiquette ARGENTINADocument3 pagesCountries' Etiquette ARGENTINAretPas encore d'évaluation
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Optimiz Ing The Membe R'S: Pation in SDC (Art Div Ision)Document7 pagesOptimiz Ing The Membe R'S: Pation in SDC (Art Div Ision)retPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Etipro Kelompok 4 (Kelas G)Document12 pagesEtipro Kelompok 4 (Kelas G)retPas encore d'évaluation
- Cleaning AgentSuppliesDocument5 pagesCleaning AgentSuppliesretPas encore d'évaluation
- Equipment HKDocument43 pagesEquipment HKretPas encore d'évaluation
- Organization ChartDocument29 pagesOrganization Chartret100% (1)
- Countries' Etiquette AFGHANISTANDocument4 pagesCountries' Etiquette AFGHANISTANretPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- 1-Introduction To Management & OrganizationDocument22 pages1-Introduction To Management & OrganizationretPas encore d'évaluation
- 3 Strategic ManagementDocument13 pages3 Strategic ManagementretPas encore d'évaluation
- FlooringDocument20 pagesFlooringretPas encore d'évaluation
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Tata Boga (India)Document5 pagesTata Boga (India)retPas encore d'évaluation
- 5-Organization Structure & DesignDocument19 pages5-Organization Structure & DesignretPas encore d'évaluation
- 9-Foundations of ControlDocument13 pages9-Foundations of ControlretPas encore d'évaluation
- 447Document10 pages447retPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- 5-Organization Structure & DesignDocument19 pages5-Organization Structure & DesignretPas encore d'évaluation
- Meeting 3Document33 pagesMeeting 3retPas encore d'évaluation
- Trail Mix Cookies IKDocument24 pagesTrail Mix Cookies IKDwi Intan WPas encore d'évaluation
- Mental Health Issues - ADHD Among ChildrenDocument9 pagesMental Health Issues - ADHD Among ChildrenFelixPas encore d'évaluation
- Notice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsDocument2 pagesNotice: Agency Information Collection Activities Proposals, Submissions, and ApprovalsJustia.comPas encore d'évaluation
- N4H InvitationLetter - FinalDocument2 pagesN4H InvitationLetter - Finalluis DiazPas encore d'évaluation
- 2018 MUSE Inspire Conference - Show and Tell SessionsDocument13 pages2018 MUSE Inspire Conference - Show and Tell SessionsMichele LambertPas encore d'évaluation
- Drug Study 1Document2 pagesDrug Study 1Hafza MacabatoPas encore d'évaluation
- Disaster Preparedness IntroDocument10 pagesDisaster Preparedness IntroBernadette-Mkandawire MandolomaPas encore d'évaluation
- Typology of Nursing Problems in Family Nursing PracticeDocument4 pagesTypology of Nursing Problems in Family Nursing PracticeLeah Abdul KabibPas encore d'évaluation
- NCLEX RN Practice Questions Set 1Document6 pagesNCLEX RN Practice Questions Set 1Jack SheperdPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Assoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyDocument8 pagesAssoc Between Poor Sleep Quality - Depression Symptoms Among ElderlyWindyanissa RecitaPas encore d'évaluation
- Lab Report 15438869 20231127064225Document1 pageLab Report 15438869 20231127064225carilloabhe21Pas encore d'évaluation
- Tea and Industrial RevolutionDocument4 pagesTea and Industrial RevolutionPhuong NguyenPas encore d'évaluation
- Nursing - Burn InjuryDocument39 pagesNursing - Burn Injuryamaracha2003Pas encore d'évaluation
- Mini Clinical Examination (Mini-CEX)Document21 pagesMini Clinical Examination (Mini-CEX)Jeffrey Dyer100% (1)
- PNA 2012 National Convention LectureDocument60 pagesPNA 2012 National Convention LectureHarby Ongbay AbellanosaPas encore d'évaluation
- Peran Perawat KomDocument27 pagesPeran Perawat Komwahyu febriantoPas encore d'évaluation
- Health Declaration FormDocument1 pageHealth Declaration FormUzair KhalidPas encore d'évaluation
- Adani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalDocument20 pagesAdani Targets Debt Cuts, Income Boost Coastal Shipping To Get Infra Status, Says SonowalboxorPas encore d'évaluation
- Disaster Nursing SAS Session 14Document6 pagesDisaster Nursing SAS Session 14Niceniadas CaraballePas encore d'évaluation
- Letters of Intent (Cover Letters)Document6 pagesLetters of Intent (Cover Letters)anca_ramona_s0% (1)
- Care ReportDocument23 pagesCare ReportSindi Muthiah UtamiPas encore d'évaluation
- Pattern Before Hospitalization During HospitalizationDocument2 pagesPattern Before Hospitalization During HospitalizationJean WinPas encore d'évaluation
- Gear Oil 85W-140: Safety Data SheetDocument7 pagesGear Oil 85W-140: Safety Data SheetsaadPas encore d'évaluation
- Fatal Airway Obstruction Due To Ludwig'sDocument6 pagesFatal Airway Obstruction Due To Ludwig'sRegina MugopalPas encore d'évaluation
- Physiological Changes Postpartum PeriodDocument2 pagesPhysiological Changes Postpartum PeriodEurielle MiolePas encore d'évaluation
- Nejmra 2023911Document8 pagesNejmra 2023911Merry LeePas encore d'évaluation
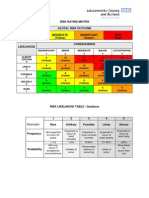
- Example of A NHS Risk Rating MatrixDocument2 pagesExample of A NHS Risk Rating MatrixRochady SetiantoPas encore d'évaluation
- Test Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDocument3 pagesTest Bank For Occupational Therapy in Mental Health A Vision For Participation 2nd Edition Catana Brown Virginia C Stoffel Jaime MunozDavid Ortiz97% (36)
- ResumeDocument4 pagesResumeAaRomalyn F. ValeraPas encore d'évaluation
- The Influence of Music in Horror Games (Final Draft)Document7 pagesThe Influence of Music in Horror Games (Final Draft)Panther LenoXPas encore d'évaluation