Vous aimerez peut-être aussi
- Printed Handout Seminar 4004 OASDocument2 pagesPrinted Handout Seminar 4004 OASArditya Dwi YudistiraPas encore d'évaluation
- Nasal Polyps Medical or Surgical ManagementDocument11 pagesNasal Polyps Medical or Surgical ManagementArditya Dwi YudistiraPas encore d'évaluation
- Printed Handout Seminar 4004 OASDocument2 pagesPrinted Handout Seminar 4004 OASArditya Dwi YudistiraPas encore d'évaluation
- Oral Findings of Systemic Lupus Erythematosus - A Grand Round CaseDocument6 pagesOral Findings of Systemic Lupus Erythematosus - A Grand Round CaseArditya Dwi YudistiraPas encore d'évaluation
- Game List.0857 3143 0030Document324 pagesGame List.0857 3143 0030Arditya Dwi YudistiraPas encore d'évaluation
- Latihan SpssDocument5 pagesLatihan SpssArditya Dwi YudistiraPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- A. Differential Diagnosis:: Bone MetastasisDocument3 pagesA. Differential Diagnosis:: Bone MetastasisDonna DumaliangPas encore d'évaluation
- Capsular Tension Rings:: Current Indications and OutcomesDocument12 pagesCapsular Tension Rings:: Current Indications and OutcomesShahid ManzoorPas encore d'évaluation
- Ebj M3 Rle24Document6 pagesEbj M3 Rle24Ayen PaloPas encore d'évaluation
- Final - HOSPITAL BILL FORMAT PDFDocument2 pagesFinal - HOSPITAL BILL FORMAT PDFH C85% (13)
- Performance of PRISM III and PELOD-2 Score in A PICUDocument6 pagesPerformance of PRISM III and PELOD-2 Score in A PICUAnantaBenvenutoPas encore d'évaluation
- Thyroid Disease in Adults PDFDocument316 pagesThyroid Disease in Adults PDFAnonymous ZZCCXMoRosPas encore d'évaluation
- Edited HP I Fri ConfDocument85 pagesEdited HP I Fri ConfTara Oliveros Dela CruzPas encore d'évaluation
- Pathophysiology For HELLP SyndromeDocument2 pagesPathophysiology For HELLP SyndromeRosemarie CarpioPas encore d'évaluation
- DR - Sreedhar CV 2018 UpdatedDocument11 pagesDR - Sreedhar CV 2018 UpdatedDr Sreedhar TirunagariPas encore d'évaluation
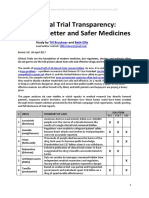
- Clinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Document21 pagesClinical Trial Transparency - A Key To Better and Safer Medicines (Till Bruckner and Beth Ellis 2017)Till BrucknerPas encore d'évaluation
- The Bamako InitiativeDocument1 pageThe Bamako InitiativekennyderayoPas encore d'évaluation
- CV 2017 VirginiaDocument4 pagesCV 2017 Virginiaapi-353693776Pas encore d'évaluation
- 1678 Using Sucralfate Tabletsto Make Enemas For Radiological Proctitis A3x2ppDocument2 pages1678 Using Sucralfate Tabletsto Make Enemas For Radiological Proctitis A3x2ppRamesh GuptaPas encore d'évaluation
- Times Leader 03-17-2013Document77 pagesTimes Leader 03-17-2013The Times LeaderPas encore d'évaluation
- MEdical Surgical REVEWERDocument86 pagesMEdical Surgical REVEWERennaedPas encore d'évaluation
- Referat Gangguan Lapang PandangDocument27 pagesReferat Gangguan Lapang PandangIkrima MuhdarmuhallyPas encore d'évaluation
- Hospitalpharmacy PDFDocument13 pagesHospitalpharmacy PDFBhavin DesaiPas encore d'évaluation
- Anna O's Significance in PsychologyDocument3 pagesAnna O's Significance in PsychologycaironsalamPas encore d'évaluation
- 2.symptoms and Signs of Psychiatric DisordersDocument53 pages2.symptoms and Signs of Psychiatric DisordersHanain Al-mahdi33% (3)
- MSN FP6216 ForsythKathryn Assessment4 2Document6 pagesMSN FP6216 ForsythKathryn Assessment4 2NbiPas encore d'évaluation
- Clinical Approach To Rapidly Progressive Renal FailureDocument6 pagesClinical Approach To Rapidly Progressive Renal FailureBryan RamseyPas encore d'évaluation
- Enteral Nutrition: Sana Inam Lecturer College of Pharmacy, GCUFDocument18 pagesEnteral Nutrition: Sana Inam Lecturer College of Pharmacy, GCUFAnum AzamPas encore d'évaluation
- Medel SonataDocument54 pagesMedel Sonatamaclab macPas encore d'évaluation
- Communication Failures An Insidious Contributor.19Document9 pagesCommunication Failures An Insidious Contributor.19Vinay GargPas encore d'évaluation
- Quality of Nursing Care Provided For PreDocument16 pagesQuality of Nursing Care Provided For PreAmmar Mustafa Mahadi AlzeinPas encore d'évaluation
- Bryan 3-24-17Document12 pagesBryan 3-24-17Bryan VandentoornPas encore d'évaluation
- Drug and Therapeutics Committee: Session 4. Assessing and Managing Medicine SafetyDocument40 pagesDrug and Therapeutics Committee: Session 4. Assessing and Managing Medicine SafetyPratyPas encore d'évaluation
- Cerumen Management PDFDocument10 pagesCerumen Management PDFHimawan WidyatmikoPas encore d'évaluation
- Hamstring StrainDocument13 pagesHamstring Strainaraaff100% (2)
- Key Aspects of State and D.C. Medical Marijuana LawsDocument16 pagesKey Aspects of State and D.C. Medical Marijuana LawsMPP100% (2)