Vous aimerez peut-être aussi
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (120)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- RS ARI-Common Cold - PPT 93Document57 pagesRS ARI-Common Cold - PPT 93Dr.P.NatarajanPas encore d'évaluation
- Abnormalities of Cortical-Limbic-Cerebellar White Matter Networks May Contribute To Treatment-Resistant Depression A Diffusion Tensor Imaging StudyDocument8 pagesAbnormalities of Cortical-Limbic-Cerebellar White Matter Networks May Contribute To Treatment-Resistant Depression A Diffusion Tensor Imaging StudyFebyPas encore d'évaluation
- Disney Princess Halloween Masquerade Masks - FDCOM PDFDocument3 pagesDisney Princess Halloween Masquerade Masks - FDCOM PDFSara ReisPas encore d'évaluation
- Structural Connectomic' Alterations in TheDocument10 pagesStructural Connectomic' Alterations in TheFebyPas encore d'évaluation
- An Introduction To Neural SystemsDocument41 pagesAn Introduction To Neural SystemsFebyPas encore d'évaluation
- Abnormalities of Cortical-Limbic-Cerebellar White Matter Networks May Contribute To Treatment-Resistant Depression A Diffusion Tensor Imaging StudyDocument8 pagesAbnormalities of Cortical-Limbic-Cerebellar White Matter Networks May Contribute To Treatment-Resistant Depression A Diffusion Tensor Imaging StudyFebyPas encore d'évaluation
- Single Agent Antihypertensive Therapy and Orthostatic Blood PressureDocument14 pagesSingle Agent Antihypertensive Therapy and Orthostatic Blood PressureFebyPas encore d'évaluation
- Contoh Final Test Dalam Bahasa InggrisDocument3 pagesContoh Final Test Dalam Bahasa InggrisnuramaliaPas encore d'évaluation
- Fundamentals - of - Caregiving - 1 PDFDocument23 pagesFundamentals - of - Caregiving - 1 PDFmoira77100% (1)
- NEERAJ KUMAR, AVTAR, (Students) JITENDER MEHLA (Research Scholar), NDRI and Dr. S.K. Sood, Senior Scientist, NDRI, KarnalDocument31 pagesNEERAJ KUMAR, AVTAR, (Students) JITENDER MEHLA (Research Scholar), NDRI and Dr. S.K. Sood, Senior Scientist, NDRI, KarnalAlokeparna RoyPas encore d'évaluation
- Communicable and Non-Communicable Diseases - of Planning (PDFDrive)Document337 pagesCommunicable and Non-Communicable Diseases - of Planning (PDFDrive)JeremiahPas encore d'évaluation
- Letter To OSHA RE: Proposed Rule Public Comments Final 2022.01.19Document15 pagesLetter To OSHA RE: Proposed Rule Public Comments Final 2022.01.19Don ParkerPas encore d'évaluation
- Ostrowska Et Al. - 2023 - Effects of Multidisciplinary Rehabilitation PrograDocument10 pagesOstrowska Et Al. - 2023 - Effects of Multidisciplinary Rehabilitation PrograIsabele Campos Costa AmaralPas encore d'évaluation
- Enicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadacheDocument5 pagesEnicillin-Like Antibiotics. Diarrhea, Nausea, Vomiting, HeadachePauline AñesPas encore d'évaluation
- Module 1 in TLE 9 WK 1 2nail CareDocument10 pagesModule 1 in TLE 9 WK 1 2nail CareAdrian AgaPas encore d'évaluation
- HODGES-Autism Spectrum Disorder Definition, Epidemiology, Causes, and Clinical EvaluationDocument11 pagesHODGES-Autism Spectrum Disorder Definition, Epidemiology, Causes, and Clinical EvaluationwPas encore d'évaluation
- WHO TRS 933 EngDocument128 pagesWHO TRS 933 EngSyed Anas GillaniPas encore d'évaluation
- Mental Health in Teens: Mata, Christine Mae Miranda, Jobelle Namoro, Jeaneth Ordas, Fatima Florian Tayco, Pam GeyserDocument9 pagesMental Health in Teens: Mata, Christine Mae Miranda, Jobelle Namoro, Jeaneth Ordas, Fatima Florian Tayco, Pam GeyserChristine Mae MataPas encore d'évaluation
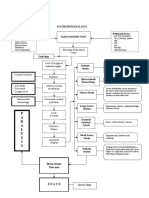
- Pathophysiology: P A R A L Y S I SDocument1 pagePathophysiology: P A R A L Y S I SJordan Garcia AguilarPas encore d'évaluation
- Foods: The Toxic Impact of Honey Adulteration: A ReviewDocument21 pagesFoods: The Toxic Impact of Honey Adulteration: A ReviewUncle RogerPas encore d'évaluation
- Impaired Posture and MovementDocument40 pagesImpaired Posture and MovementMohamed Magdy ElMeligiePas encore d'évaluation
- Sirwan Ali Enterohemorrhagic-Escherichia-coliDocument8 pagesSirwan Ali Enterohemorrhagic-Escherichia-coliDlzar AbubakrPas encore d'évaluation
- Uddeholms Ab Safety Data Sheet: UDDEHOLM (BRUSH WELLMAN) Alloys: Moldmax®HH/LH and Weldpak®Document8 pagesUddeholms Ab Safety Data Sheet: UDDEHOLM (BRUSH WELLMAN) Alloys: Moldmax®HH/LH and Weldpak®awesome_600Pas encore d'évaluation
- PathoDocument2 pagesPathohrry stylesPas encore d'évaluation
- PIEPIEDocument23 pagesPIEPIEJaycee NodadoPas encore d'évaluation
- Congenital Heart Disease: Education and Practice GapsDocument18 pagesCongenital Heart Disease: Education and Practice GapsAlvaro Ignacio Lagos SuilPas encore d'évaluation
- GeneticTestPdf 6538 PDFDocument21 pagesGeneticTestPdf 6538 PDFMarianaBBazanPas encore d'évaluation
- Mathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesDocument23 pagesMathematical Modeling of COVID-19 Spreading With Asymptomatic Infected and Interacting PeoplesYjhvhgjvPas encore d'évaluation
- Stress Symptom Checklist: Physical Symptoms Psychological SymptomsDocument1 pageStress Symptom Checklist: Physical Symptoms Psychological Symptomsmaria pia otarolaPas encore d'évaluation
- Activity Intolerance NCPDocument7 pagesActivity Intolerance NCPamitPas encore d'évaluation
- Lumber Mold - WPPA - Mold-Housing-Wood-Tg2Document12 pagesLumber Mold - WPPA - Mold-Housing-Wood-Tg2Jeff HPas encore d'évaluation
- Human DevelopmentDocument13 pagesHuman DevelopmentmysterioushumanePas encore d'évaluation
- Labor Code of The Philippines Volume I - Book 4Document144 pagesLabor Code of The Philippines Volume I - Book 4Joanne CamacamPas encore d'évaluation
- Pancreatic Function TestsDocument12 pagesPancreatic Function TestsDhera CharlesPas encore d'évaluation
- BibliographyDocument2 pagesBibliographyapi-255681450Pas encore d'évaluation
- Various CT Scan Score in Pneumonia and CovidDocument8 pagesVarious CT Scan Score in Pneumonia and CovidrishaPas encore d'évaluation