Vous aimerez peut-être aussi
- Phdthesisow RGDocument85 pagesPhdthesisow RGAstrit E. Salihu100% (1)
- Optimization of Water Supply System Using Software EPANET 2.0Document10 pagesOptimization of Water Supply System Using Software EPANET 2.0Astrit E. SalihuPas encore d'évaluation
- 2023 Calendar MonthsDocument1 page2023 Calendar MonthsAstrit E. SalihuPas encore d'évaluation
- Technical Notes: Reducing Erosional Impacts of RoadsDocument27 pagesTechnical Notes: Reducing Erosional Impacts of RoadsAstrit E. SalihuPas encore d'évaluation
- Të Dhënat: Nga Tabelat Prof. Branko Zidersic LexojmDocument4 pagesTë Dhënat: Nga Tabelat Prof. Branko Zidersic LexojmAstrit E. SalihuPas encore d'évaluation
- Bhanu Paperfor HydroDocument11 pagesBhanu Paperfor HydroAstrit E. SalihuPas encore d'évaluation
- PSH Map CoordinateDocument1 pagePSH Map CoordinateAstrit E. SalihuPas encore d'évaluation
- Water Flow Meters Measure Up To 300mm DiameterDocument3 pagesWater Flow Meters Measure Up To 300mm DiameterAstrit E. SalihuPas encore d'évaluation
- Water: Swimming Pool Evaporative Water Loss and Water Use in The Balearic Islands (Spain)Document19 pagesWater: Swimming Pool Evaporative Water Loss and Water Use in The Balearic Islands (Spain)jp taghapPas encore d'évaluation
- School Sewage Network DiagramDocument9 pagesSchool Sewage Network DiagramAstrit E. SalihuPas encore d'évaluation
- Webtv ListDocument200 pagesWebtv ListAstrit E. SalihuPas encore d'évaluation
- The - Maximum Ow Model With Uncertain Capacities: Applied Mathematical Modelling April 2015Document9 pagesThe - Maximum Ow Model With Uncertain Capacities: Applied Mathematical Modelling April 2015Astrit E. SalihuPas encore d'évaluation
- EU Guidelines PDFDocument59 pagesEU Guidelines PDFtimky8Pas encore d'évaluation
- Mathtype 7Document1 pageMathtype 7Astrit E. SalihuPas encore d'évaluation
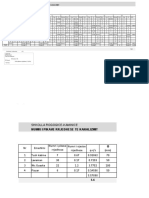
- Shkolla E Mesme Rogoqice-Kaminice: Caktimi I Njesive Rrjedhese Për UjësjellësDocument11 pagesShkolla E Mesme Rogoqice-Kaminice: Caktimi I Njesive Rrjedhese Për UjësjellësAstrit E. SalihuPas encore d'évaluation
- Water: Swimming Pool Evaporative Water Loss and Water Use in The Balearic Islands (Spain)Document19 pagesWater: Swimming Pool Evaporative Water Loss and Water Use in The Balearic Islands (Spain)jp taghapPas encore d'évaluation
- 2006 Floods in The Danube River Basin WWF Working PaperDocument41 pages2006 Floods in The Danube River Basin WWF Working PaperAstrit E. SalihuPas encore d'évaluation
- Sustainability 05 03060Document17 pagesSustainability 05 03060Astrit E. SalihuPas encore d'évaluation
- Ects Name:: Hydrology and Hydraulic Structures 9Document1 pageEcts Name:: Hydrology and Hydraulic Structures 9Astrit E. SalihuPas encore d'évaluation
- WideDocument15 pagesWideAstrit E. SalihuPas encore d'évaluation
- Au 7 0054 00326 - 1Document5 pagesAu 7 0054 00326 - 1Astrit E. SalihuPas encore d'évaluation
- AK47Document42 pagesAK47Astrit E. SalihuPas encore d'évaluation
- Sensors 09 06411Document24 pagesSensors 09 06411Arun RajaPas encore d'évaluation
- WB p151026 NegyxjaDocument159 pagesWB p151026 NegyxjaAstrit E. SalihuPas encore d'évaluation
- Pub Earth Amp Rockfill DamsDocument342 pagesPub Earth Amp Rockfill DamsAstrit E. SalihuPas encore d'évaluation
- Water Pollution in KosovoDocument42 pagesWater Pollution in KosovoAstrit E. SalihuPas encore d'évaluation
- En TypologieDocument21 pagesEn TypologieAstrit E. SalihuPas encore d'évaluation
- 02 ShalaDocument10 pages02 ShalaAstrit E. SalihuPas encore d'évaluation
- Urn NBN Si Doc Eh24curqDocument6 pagesUrn NBN Si Doc Eh24curqAstrit E. SalihuPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5784)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (890)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (587)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (265)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (72)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (119)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Mar For M: I MMQ SeriesDocument28 pagesMar For M: I MMQ SeriesIpal Febri NartaPas encore d'évaluation
- NTE56004 Thru NTE56010 TRIAC, 15 Amp: FeaturesDocument2 pagesNTE56004 Thru NTE56010 TRIAC, 15 Amp: FeaturesFreddy SarabiaPas encore d'évaluation
- Dr. Blyden: Chronic Obstructive Pulmonary Disease (Copd)Document63 pagesDr. Blyden: Chronic Obstructive Pulmonary Disease (Copd)Blyden NoahPas encore d'évaluation
- Dokumen - Tips - Astm A535 9 Percent NickelDocument5 pagesDokumen - Tips - Astm A535 9 Percent NickelJeovanne CabralPas encore d'évaluation
- SAFETY AND LOSS PREVENTION FOR CHEMICAL PROCESS FACILITIESDocument13 pagesSAFETY AND LOSS PREVENTION FOR CHEMICAL PROCESS FACILITIESKinosraj KumaranPas encore d'évaluation
- Demo DLLDocument2 pagesDemo DLLArlene Diokno100% (1)
- Refraction Through Lenses & Optical Instruments5Document144 pagesRefraction Through Lenses & Optical Instruments5geniusamahPas encore d'évaluation
- Akshay 71 Seminar ReportDocument22 pagesAkshay 71 Seminar ReportSanket Yadav25% (4)
- Manual of Curatorship: A Guide To Museum PracticeDocument7 pagesManual of Curatorship: A Guide To Museum PracticeLuísa MenezesPas encore d'évaluation
- Classification of Placenta PDFDocument5 pagesClassification of Placenta PDFAdarsh jainPas encore d'évaluation
- HHG4M - Lifespan Development Textbook Lesson 4Document88 pagesHHG4M - Lifespan Development Textbook Lesson 4Lubomira SucheckiPas encore d'évaluation
- CERT Basic Training Participant Manual - 2011Document332 pagesCERT Basic Training Participant Manual - 2011jegodfreyPas encore d'évaluation
- Ch1 PDFDocument54 pagesCh1 PDFChristian Jegues100% (2)
- Quant One Analyser – endless possibilitiesDocument6 pagesQuant One Analyser – endless possibilitiesSamuel SuPas encore d'évaluation
- Diabetic Safe - One Pager - Version 1.0 - Oct 20Document2 pagesDiabetic Safe - One Pager - Version 1.0 - Oct 20naval730107Pas encore d'évaluation
- Type 2 Diabetes MellitusDocument6 pagesType 2 Diabetes MellitusJoy NisoladaPas encore d'évaluation
- Lab 1 Free Fall GEC - CEA21 - OERSTEDDocument6 pagesLab 1 Free Fall GEC - CEA21 - OERSTEDLee-Ann LimPas encore d'évaluation
- Kaustubh Laturkar Fuel Cell ReportDocument3 pagesKaustubh Laturkar Fuel Cell Reportkos19188Pas encore d'évaluation
- Production Management Midterm ReviewDocument21 pagesProduction Management Midterm Reviewielsiu21184Pas encore d'évaluation
- Module 6 - FormworksDocument8 pagesModule 6 - FormworksAldrich Francis Ortiz Peñaflor100% (1)
- LTE Speech Traffic Dimenshioning For VoipDocument6 pagesLTE Speech Traffic Dimenshioning For VoipRahul GuptaPas encore d'évaluation
- 3.1-T.C.Dies PDFDocument6 pages3.1-T.C.Dies PDFYahyaMoummouPas encore d'évaluation
- ASME B31.4-2016 Pipeline Transportation Systems For Liquids and SlurriesDocument1 pageASME B31.4-2016 Pipeline Transportation Systems For Liquids and SlurriesJose Rodrigo Salguero DuranPas encore d'évaluation
- AAA Variable Spring Hangers CatalogDocument31 pagesAAA Variable Spring Hangers CatalogNopparut0% (1)
- Diff Types of Transmission Lines Used in CommsDocument9 pagesDiff Types of Transmission Lines Used in CommsLe AndroPas encore d'évaluation
- NQ-NQM Panelboards and Qonq Load Centers Information Manual 80043-712-06 Rev.02 06-2015 2 PiezasDocument144 pagesNQ-NQM Panelboards and Qonq Load Centers Information Manual 80043-712-06 Rev.02 06-2015 2 PiezasNadia EspinozaPas encore d'évaluation
- Gas Turbine Performance Enhancement Update: GE Energy ServicesDocument45 pagesGas Turbine Performance Enhancement Update: GE Energy Servicesesteban100% (1)
- 2 History of OrthodonticsDocument11 pages2 History of OrthodonticsMeiz JaleelPas encore d'évaluation
- Variants of NormalDocument9 pagesVariants of NormalFaizah HannyPas encore d'évaluation
- EAGLE TUGS - Parts Service ManualDocument72 pagesEAGLE TUGS - Parts Service ManualDave MilnerPas encore d'évaluation