Vous aimerez peut-être aussi
- Occupation Analysis in PracticeD'EverandOccupation Analysis in PracticeLynette MackenziePas encore d'évaluation
- Occupational Therapy and Life Course Development: A Work Book for Professional PracticeD'EverandOccupational Therapy and Life Course Development: A Work Book for Professional PracticePas encore d'évaluation
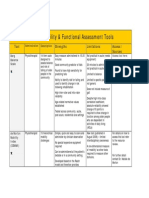
- Mobility and Functional Assessment ToolsDocument4 pagesMobility and Functional Assessment Toolssonya63265Pas encore d'évaluation
- GmfmscoresheetDocument6 pagesGmfmscoresheetapi-260049180Pas encore d'évaluation
- Weefim Score Sheet: Brain InjuryDocument3 pagesWeefim Score Sheet: Brain InjuryDiedeePas encore d'évaluation
- LABORATORY PRACTICE: Range of Motion WorksheetDocument12 pagesLABORATORY PRACTICE: Range of Motion WorksheetMike ConnorsPas encore d'évaluation
- Dyssemia Rating ScaleDocument8 pagesDyssemia Rating ScaleHazardous7Pas encore d'évaluation
- Peabody y Movent ABCDocument11 pagesPeabody y Movent ABCIngrid BarkoPas encore d'évaluation
- Pediatric Wheelchair Toolkit FINALDocument6 pagesPediatric Wheelchair Toolkit FINALIndiana Family to FamilyPas encore d'évaluation
- 892 Physiotherapy Management of Paediatric Flat FeetDocument20 pages892 Physiotherapy Management of Paediatric Flat FeetCalvina Mizumi100% (1)
- Spinal Cord Assesment Form PTDocument8 pagesSpinal Cord Assesment Form PTSureaka PonnusamyPas encore d'évaluation
- Occt 526 - Child-Based PicoDocument14 pagesOcct 526 - Child-Based Picoapi-291380671Pas encore d'évaluation
- Activity Analysis, Creativity and Playfulness in Pediatric Occupational TherapyDocument16 pagesActivity Analysis, Creativity and Playfulness in Pediatric Occupational TherapySofia VieiraPas encore d'évaluation
- OTB 502 Syllabus 2019Document22 pagesOTB 502 Syllabus 2019Gehan BotorsPas encore d'évaluation
- NDTDocument9 pagesNDTKhaing Hsu WaiPas encore d'évaluation
- ACIS - Interpersonal InteractionsDocument1 pageACIS - Interpersonal InteractionsangelulisPas encore d'évaluation
- Rubric Mini PracticalDocument2 pagesRubric Mini PracticalAigen OcampoPas encore d'évaluation
- PT GoalsDocument13 pagesPT Goalsnaomi harowPas encore d'évaluation
- Uniform Terminology AOTA PDFDocument8 pagesUniform Terminology AOTA PDFLaura GuevaraPas encore d'évaluation
- Mosey's Developmental GroupsDocument3 pagesMosey's Developmental Groupsedwin.roc523100% (2)
- PANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstoneDocument44 pagesPANat - Thetrical - Air Splints - Talas Pneumaticas Margaret JohnstonePedro GouveiaPas encore d'évaluation
- Neuro-Developmental Therapy/Treatment: Pediatric Physical Therapy, NDTDocument13 pagesNeuro-Developmental Therapy/Treatment: Pediatric Physical Therapy, NDTMuhamed Elsayed - Zalat100% (1)
- Hand FunctionDocument37 pagesHand FunctionPrince Raj SinhaPas encore d'évaluation
- Video Modeling and Observational Learning To Teach Gaming Access To Students With ASDDocument14 pagesVideo Modeling and Observational Learning To Teach Gaming Access To Students With ASDMaria Elisa Granchi FonsecaPas encore d'évaluation
- 遊戲藝術卡 (英文說明)Document4 pages遊戲藝術卡 (英文說明)台灣藝術治療學會Pas encore d'évaluation
- Wota2: Water Orientation Test Alyn 2Document2 pagesWota2: Water Orientation Test Alyn 2Sergio CurteanPas encore d'évaluation
- Satco Clinical WorkbookDocument6 pagesSatco Clinical WorkbookKidz to Adultz Exhibitions100% (1)
- Cerebral Palsy SlidesDocument22 pagesCerebral Palsy Slidesapi-301967651Pas encore d'évaluation
- Post Stroke Functional Exercises For RehabilitationDocument37 pagesPost Stroke Functional Exercises For Rehabilitationjoel_simon_23100% (1)
- GMFMDocument1 pageGMFMFlorin Dragos Caprita100% (1)
- 2 Introduction To TheoryDocument14 pages2 Introduction To TheoryNurul Izzah Wahidul AzamPas encore d'évaluation
- Guidelines For Documentation of Occupational Therapy PDFDocument7 pagesGuidelines For Documentation of Occupational Therapy PDFMaria AiramPas encore d'évaluation
- The Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityDocument7 pagesThe Effect of Co-Op Approach in Improving Visual Motor Integration Skills in Children With Learning DisabilityIJAR JOURNALPas encore d'évaluation
- Autism DefinitionDocument2 pagesAutism Definitionapi-213387477Pas encore d'évaluation
- Knox Prescool PlayDocument7 pagesKnox Prescool Playkonna4539Pas encore d'évaluation
- Wolf Motor Function TestDocument23 pagesWolf Motor Function TestSai RamPas encore d'évaluation
- Ota Group ProtocolDocument26 pagesOta Group Protocolapi-318685839Pas encore d'évaluation
- 2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)Document54 pages2001 Candidate Handbook: National Board For Certification in Occupational Therapy, Inc. (Nbcot)engshi18Pas encore d'évaluation
- Normalisation Process Theory A Framework For Developing, Evaluating and Implementing Complex InterventionsDocument12 pagesNormalisation Process Theory A Framework For Developing, Evaluating and Implementing Complex InterventionsTran Ngoc TienPas encore d'évaluation
- FIM ManualDocument24 pagesFIM ManualAnshuman MihirPas encore d'évaluation
- Aota Professional Development Tool SheetDocument2 pagesAota Professional Development Tool Sheetapi-382638519Pas encore d'évaluation
- Treating FeadingDocument126 pagesTreating FeadingTerapie AbaPas encore d'évaluation
- Application of Facilitatory Approaches in Developmental DysarthriaDocument22 pagesApplication of Facilitatory Approaches in Developmental Dysarthriakeihoina keihoinaPas encore d'évaluation
- Chapter 8Document30 pagesChapter 8Karla CarazoPas encore d'évaluation
- Benchmarking: An International Journal: Emerald Article: Kpis: A Critical Appraisal of Their Use in ConstructionDocument26 pagesBenchmarking: An International Journal: Emerald Article: Kpis: A Critical Appraisal of Their Use in ConstructionJojo LamPas encore d'évaluation
- Motor MildstonesDocument13 pagesMotor MildstonesVaio Wolff AbendrothPas encore d'évaluation
- Occupational Therapy As A Major Activity of Human Being: by Rafia KhalidDocument20 pagesOccupational Therapy As A Major Activity of Human Being: by Rafia Khalidnomi9818Pas encore d'évaluation
- General Self-Efficacy Scale (GSE)Document2 pagesGeneral Self-Efficacy Scale (GSE)Angelus MorePas encore d'évaluation
- CIMT ManualDocument48 pagesCIMT ManualExternal100% (1)
- B P O M: Rachial Lexus Utcome EasureDocument14 pagesB P O M: Rachial Lexus Utcome EasureVirginia Feren FraganzhaPas encore d'évaluation
- Occupational AdaptationDocument5 pagesOccupational AdaptationVASH12345100% (1)
- Growth and DevelopmentDocument2 pagesGrowth and DevelopmentCharmaine Vergara - GementizaPas encore d'évaluation
- Troxipide vs. Rabeprazole in The Treatment of GastritisDocument8 pagesTroxipide vs. Rabeprazole in The Treatment of GastritisZuventusHealthcarePas encore d'évaluation
- OT - Milestone RetypedDocument6 pagesOT - Milestone RetypedAubrey Vale SagunPas encore d'évaluation
- Aota Professional Development ToolDocument2 pagesAota Professional Development Toolapi-339174797Pas encore d'évaluation
- Occupational Therapy Examination Review Guide 4th Edition Ebook PDFDocument57 pagesOccupational Therapy Examination Review Guide 4th Edition Ebook PDFrobert.campbell485Pas encore d'évaluation
- 56 (Bobath Concept)Document14 pages56 (Bobath Concept)SardarChangezKhan100% (1)
- INCLEN Diagnostic Tool For Attention Deficit Hyperactive Disorder INDT ADHDDocument5 pagesINCLEN Diagnostic Tool For Attention Deficit Hyperactive Disorder INDT ADHDNaseeba FaburikagePas encore d'évaluation
- A.5 Assessment PowerPoint 2016Document38 pagesA.5 Assessment PowerPoint 2016Ptrc Lbr LpPas encore d'évaluation
- The Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionD'EverandThe Multicontext Approach to Cognitive Rehabilitation: A Metacognitive Strategy Intervention to Optimize Functional CognitionPas encore d'évaluation
- Australian ACE-III Administration and Scoring GuideDocument10 pagesAustralian ACE-III Administration and Scoring GuideLydia MartínPas encore d'évaluation
- ACE-III Administration (UK)Document6 pagesACE-III Administration (UK)Livgian KaurPas encore d'évaluation
- Assessment Living SkillsDocument8 pagesAssessment Living SkillsLydia MartínPas encore d'évaluation
- Assessment Living SkillsDocument8 pagesAssessment Living SkillsLydia MartínPas encore d'évaluation
- Attitudes Toward Disabled PeopleDocument2 pagesAttitudes Toward Disabled PeopleLydia Martín100% (7)
- Amputee Activity Score PDFDocument5 pagesAmputee Activity Score PDFLydia MartínPas encore d'évaluation
- Short Physical Performance BatteryDocument3 pagesShort Physical Performance BatteryLydia MartínPas encore d'évaluation
- Execution Function Perfor Test PDFDocument21 pagesExecution Function Perfor Test PDFLydia MartínPas encore d'évaluation
- Amputee Activity ScoreDocument5 pagesAmputee Activity ScoreLydia MartínPas encore d'évaluation
- Knox Preschool Play ScaleDocument3 pagesKnox Preschool Play ScaleLydia Martín93% (15)
- OT Serv in Psych and Social Aspects of MHDocument19 pagesOT Serv in Psych and Social Aspects of MHLydia MartínPas encore d'évaluation
- The Concise 48 Laws of Power PDFDocument203 pagesThe Concise 48 Laws of Power PDFkaran kamath100% (1)
- Asymetry Analysis of Breast Thermograma Using Automated SegmentationDocument8 pagesAsymetry Analysis of Breast Thermograma Using Automated Segmentationazazel17Pas encore d'évaluation
- NCLEX 20QUESTIONS 20safety 20and 20infection 20controlDocument8 pagesNCLEX 20QUESTIONS 20safety 20and 20infection 20controlCassey MillanPas encore d'évaluation
- Persephone by Julia Donaldson: (A Meadow. Enters Persephone, Picking The Petals of A Daisy.)Document10 pagesPersephone by Julia Donaldson: (A Meadow. Enters Persephone, Picking The Petals of A Daisy.)Dobler Liliana100% (1)
- Zoe LeonardDocument9 pagesZoe LeonardSandro Alves SilveiraPas encore d'évaluation
- Vlue AdDocument153 pagesVlue AdsindhushankarPas encore d'évaluation
- DBI Setup Steps For Procurement IntelligenceDocument4 pagesDBI Setup Steps For Procurement IntelligenceAnubhav.MittalPas encore d'évaluation
- Accounting TheoryDocument192 pagesAccounting TheoryABDULLAH MOHAMMEDPas encore d'évaluation
- First Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldDocument25 pagesFirst Quarter-Module 2-Lesson 2-21st Century Literature From The Philippines and The WorldAndrea Ibañez73% (11)
- NursesExperiencesofGriefFollowing28 8 2017thepublishedDocument14 pagesNursesExperiencesofGriefFollowing28 8 2017thepublishedkathleen PerezPas encore d'évaluation
- Adult Consensual SpankingDocument21 pagesAdult Consensual Spankingswl156% (9)
- Sample Opposition To Motion To Alter or Amend Judgment in United States District CourtDocument3 pagesSample Opposition To Motion To Alter or Amend Judgment in United States District CourtStan BurmanPas encore d'évaluation
- Lolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad MedinaceliDocument3 pagesLolita Enrico Vs Heirs of Spouses Eulogio Medinaceli and Trinidad Medinacelichatmche-06Pas encore d'évaluation
- MODULE 13 Ethics Through Thick and ThinDocument7 pagesMODULE 13 Ethics Through Thick and ThinCristobal M. CantorPas encore d'évaluation
- English Preparation Guide DAF 202306Document12 pagesEnglish Preparation Guide DAF 202306TIexamesPas encore d'évaluation
- VlsiDocument216 pagesVlsisenthil_5Pas encore d'évaluation
- Academic Calendar 2014 15Document6 pagesAcademic Calendar 2014 15D Geetha DuraiPas encore d'évaluation
- Cleric Spell List D&D 5th EditionDocument9 pagesCleric Spell List D&D 5th EditionLeandros Mavrokefalos100% (2)
- Fsi GreekBasicCourse Volume1 StudentTextDocument344 pagesFsi GreekBasicCourse Volume1 StudentTextbudapest1Pas encore d'évaluation
- Watchitv Portable: Iptv Expert Analysis Application: Key ApplicationsDocument5 pagesWatchitv Portable: Iptv Expert Analysis Application: Key ApplicationsBen PoovinPas encore d'évaluation
- EmTech TG Acad v5 112316Document87 pagesEmTech TG Acad v5 112316Arvin Barrientos Bernesto67% (3)
- Lee Gwan Cheung Resume WeeblyDocument1 pageLee Gwan Cheung Resume Weeblyapi-445443446Pas encore d'évaluation
- Rule 107Document8 pagesRule 107AlexPas encore d'évaluation
- Hinog vs. MellicorDocument11 pagesHinog vs. MellicorGreta VilarPas encore d'évaluation
- Philippine Psychometricians Licensure Exam RevieweDocument1 pagePhilippine Psychometricians Licensure Exam RevieweKristelle Mae C. Azucenas0% (1)
- Exercise On Relative ClausesDocument5 pagesExercise On Relative ClausesSAmuel QuinteroPas encore d'évaluation
- Theory of Interpersonal RelationsDocument2 pagesTheory of Interpersonal RelationsAra Gayares Gallo100% (1)
- EC SF Presentation 02Document10 pagesEC SF Presentation 02Ahmed NafeaPas encore d'évaluation
- India Internet Goldman SachsDocument86 pagesIndia Internet Goldman SachsTaranjeet SinghPas encore d'évaluation
- Classics and The Atlantic Triangle - Caribbean Readings of Greece and Rome Via AfricaDocument12 pagesClassics and The Atlantic Triangle - Caribbean Readings of Greece and Rome Via AfricaAleja KballeroPas encore d'évaluation