Vous aimerez peut-être aussi
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- In Vitro Fertilization - Report - g8Document20 pagesIn Vitro Fertilization - Report - g8Maica GeePas encore d'évaluation
- Fertility Clinic Business Plan TemplateDocument7 pagesFertility Clinic Business Plan TemplateAhmed M. Rafat100% (1)
- Performance of First Trimester Fetal Ultrasound ScanDocument12 pagesPerformance of First Trimester Fetal Ultrasound ScanPujianti LestarinaPas encore d'évaluation
- EMQs For The MRCOG Part 2-The Essential GuideDocument152 pagesEMQs For The MRCOG Part 2-The Essential GuideJuanda Raynaldi100% (1)
- Multiple-Choice Questions: Paper 2: A B C D eDocument35 pagesMultiple-Choice Questions: Paper 2: A B C D eCher'ieie'sa RifirandaPas encore d'évaluation
- Recurrent Implantation Failure-Update Overview OnDocument19 pagesRecurrent Implantation Failure-Update Overview Onn2763288100% (1)
- Hyperemesis GravidarumDocument7 pagesHyperemesis GravidarumPrawira Weka AkbariPas encore d'évaluation
- Guidelines Ovarian CancerDocument78 pagesGuidelines Ovarian CancerCher'ieie'sa RifirandaPas encore d'évaluation
- A Prediction Score For Safe and Successful Vaginal Birth After Cesarean Delivery A Prospective Controlled Study 2167 0420.1000129Document7 pagesA Prediction Score For Safe and Successful Vaginal Birth After Cesarean Delivery A Prospective Controlled Study 2167 0420.1000129Cher'ieie'sa RifirandaPas encore d'évaluation
- Syndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityDocument5 pagesSyndrome of Newborn: Versus: THE Respiratory Distress THE Immaturity PrematurityCher'ieie'sa RifirandaPas encore d'évaluation
- 19 Pengukuran Dalam PenelitianDocument7 pages19 Pengukuran Dalam PenelitianCher'ieie'sa RifirandaPas encore d'évaluation
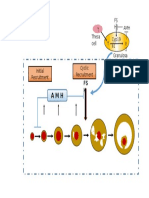
- T Cyp19 A1 T Theca Cell FS H AMHDocument1 pageT Cyp19 A1 T Theca Cell FS H AMHCher'ieie'sa RifirandaPas encore d'évaluation
- An Care Tutor 20 DecDocument75 pagesAn Care Tutor 20 DecCher'ieie'sa RifirandaPas encore d'évaluation
- Foot UlcersDocument29 pagesFoot UlcersCher'ieie'sa RifirandaPas encore d'évaluation
- Rymer CHPT 01-29a40fc0rdzDocument29 pagesRymer CHPT 01-29a40fc0rdzCher'ieie'sa RifirandaPas encore d'évaluation
- Stevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Topical Treatment Influencing Systemic ResponseDocument8 pagesStevens-Johnson Syndrome and Toxic Epidermal Necrolysis: Topical Treatment Influencing Systemic ResponseCher'ieie'sa RifirandaPas encore d'évaluation
- Stem Cell Argumentative EssayDocument10 pagesStem Cell Argumentative EssayNafisa Afsana Taskia100% (3)
- Sperm Recovery and SurvivalDocument6 pagesSperm Recovery and SurvivalArturo IturraldePas encore d'évaluation
- IVF Family Law IDocument8 pagesIVF Family Law IJaishree KaushikPas encore d'évaluation
- Seeds of Innocence To Add 20 IVF & Fertility Centres Across India by FY22 - The Economic TimesDocument3 pagesSeeds of Innocence To Add 20 IVF & Fertility Centres Across India by FY22 - The Economic TimessidPas encore d'évaluation
- Ectopic Pregnancy - MedscapeDocument31 pagesEctopic Pregnancy - Medscapeantonio91uPas encore d'évaluation
- Sperm DNA Integrity Does Play A Crucial Role For Embryo Development After ICSI, Notably When Good Quality Oocytes From Young Donors Are UsedDocument14 pagesSperm DNA Integrity Does Play A Crucial Role For Embryo Development After ICSI, Notably When Good Quality Oocytes From Young Donors Are UsedCandidaPas encore d'évaluation
- Human Menopausal Gonadotropins (HMG) : Coverage RationaleDocument11 pagesHuman Menopausal Gonadotropins (HMG) : Coverage RationaleMahmoud El MohamdyPas encore d'évaluation
- 2nd National Moot On Surrogacy LawDocument22 pages2nd National Moot On Surrogacy LawXyzPas encore d'évaluation
- Best Practice & Research Clinical Obstetrics and GynaecologyDocument12 pagesBest Practice & Research Clinical Obstetrics and GynaecologyGrit WingsPas encore d'évaluation
- FCL6 - Midterm Issues in Human SocietyDocument19 pagesFCL6 - Midterm Issues in Human SocietyJamaeca A EdraPas encore d'évaluation
- IVF - Molecular Filtration For Life - ENDocument8 pagesIVF - Molecular Filtration For Life - ENSergei KurpishPas encore d'évaluation
- AIA ProhealthDocument18 pagesAIA ProhealthHihiPas encore d'évaluation
- Non-Conventional Method of Procreation - Paternity and FiliationDocument3 pagesNon-Conventional Method of Procreation - Paternity and Filiationgrisaille delasalasPas encore d'évaluation
- Daily MNGT Plan3Document4 pagesDaily MNGT Plan3Christian Apple Angwas GonzalesPas encore d'évaluation
- Drugs in Sport EssayDocument5 pagesDrugs in Sport Essaysbbftinbf100% (2)
- Das Handy in Der SchuleDocument11 pagesDas Handy in Der Schuleandi hamatajPas encore d'évaluation
- Subfertility: Definition and ClassificationsDocument18 pagesSubfertility: Definition and ClassificationsAnonymous 0C4OZmRPas encore d'évaluation
- M U Ltifeta L Pregnancy: Mechanisms of Multifetal GestationsDocument43 pagesM U Ltifeta L Pregnancy: Mechanisms of Multifetal GestationsyayayanizaPas encore d'évaluation
- Science and The LeftDocument20 pagesScience and The LeftPeggy W SatterfieldPas encore d'évaluation
- The Economist UK Edition - July 22 2023Document94 pagesThe Economist UK Edition - July 22 2023ruoxuemiPas encore d'évaluation
- ZIFT FinalDocument11 pagesZIFT Finalblese56100% (1)
- InfertilityDocument11 pagesInfertilityBee LeriosPas encore d'évaluation
- 3 Tests For Madrid PDFDocument7 pages3 Tests For Madrid PDFanon_336126331Pas encore d'évaluation
- SURROGACYDocument9 pagesSURROGACYJAYA MISHRAPas encore d'évaluation
- Recommendations of The Expert Panel On Infertility and AdoptionDocument229 pagesRecommendations of The Expert Panel On Infertility and AdoptionThe Globe and MailPas encore d'évaluation
- 1 s2.0 S2352552523000117 MainDocument10 pages1 s2.0 S2352552523000117 MainTahani MoncerPas encore d'évaluation