Vous aimerez peut-être aussi
- PTERIGIUM (Nadia) - DR - GILBERTDocument11 pagesPTERIGIUM (Nadia) - DR - GILBERTYoga WitularPas encore d'évaluation
- MotivaasiDocument1 pageMotivaasiYoga WitularPas encore d'évaluation
- Regio Dorsum Manus DextraDocument1 pageRegio Dorsum Manus DextraYoga WitularPas encore d'évaluation
- Daftar Pustaka PRDocument1 pageDaftar Pustaka PRYoga WitularPas encore d'évaluation
- Daftar PustakaDocument2 pagesDaftar PustakaYoga WitularPas encore d'évaluation
- Daftar Pustaka MavDocument1 pageDaftar Pustaka MavYoga WitularPas encore d'évaluation
- Status Kalazion - Yoga 1161050136Document10 pagesStatus Kalazion - Yoga 1161050136Yoga WitularPas encore d'évaluation
- Status Kalazion - Yoga 1161050136Document10 pagesStatus Kalazion - Yoga 1161050136Yoga WitularPas encore d'évaluation
- Daftar Pustaka MavDocument1 pageDaftar Pustaka MavYoga WitularPas encore d'évaluation
- Daftar Pustaka CA MammaeDocument1 pageDaftar Pustaka CA MammaeYoga WitularPas encore d'évaluation
- JadadajdajkdjsdjfdbsjkfdsfbdfDocument1 pageJadadajdajkdjsdjfdbsjkfdsfbdfYoga WitularPas encore d'évaluation
- Status Kalazion - Yoga 1161050136Document10 pagesStatus Kalazion - Yoga 1161050136Yoga WitularPas encore d'évaluation
- JadadajdajkdjsdjfdbsjkfdsfbdfDocument1 pageJadadajdajkdjsdjfdbsjkfdsfbdfYoga WitularPas encore d'évaluation
- NXNVXCVCXVXCVNXCVNDocument1 pageNXNVXCVCXVXCVNXCVNYoga WitularPas encore d'évaluation
- STATUS UJIAN MATA Risda in Englishss FixDocument5 pagesSTATUS UJIAN MATA Risda in Englishss FixYoga WitularPas encore d'évaluation
- Daftar Pustaka TrikomoniasisDocument3 pagesDaftar Pustaka TrikomoniasisYoga WitularPas encore d'évaluation
- Pterigium (Nadia) - DR - GilbertDocument11 pagesPterigium (Nadia) - DR - GilbertYoga WitularPas encore d'évaluation
- Chlamydia SlidesDocument63 pagesChlamydia SlidesEspecialistaLanderPas encore d'évaluation
- Daftar Pustaka TrikomoniasisDocument3 pagesDaftar Pustaka TrikomoniasisYoga WitularPas encore d'évaluation
- Fisiologi HemodinamikaDocument11 pagesFisiologi HemodinamikaYoga WitularPas encore d'évaluation
- Daftar Pustaka MavDocument1 pageDaftar Pustaka MavYoga WitularPas encore d'évaluation
- HttpsDocument1 pageHttpsYoga WitularPas encore d'évaluation
- Daftar Pustaka MavDocument1 pageDaftar Pustaka MavYoga WitularPas encore d'évaluation
- Dr. Jusuf Wijaya - StrabismusDocument32 pagesDr. Jusuf Wijaya - StrabismusGerry SanjayaPas encore d'évaluation
- Dr. Demak - HIV TestDocument36 pagesDr. Demak - HIV TestMichael TambunanPas encore d'évaluation
- Biochemical Aspects of Drowning Impacts (Januari 2015)Document21 pagesBiochemical Aspects of Drowning Impacts (Januari 2015)Yoga WitularPas encore d'évaluation
- SampahDocument1 pageSampahYoga WitularPas encore d'évaluation
- Splanchnopleure vs. Somatopleure: I) DefinitionsDocument1 pageSplanchnopleure vs. Somatopleure: I) DefinitionsYoga WitularPas encore d'évaluation
- Dr. Demak - HIV TestDocument36 pagesDr. Demak - HIV TestMichael TambunanPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Nail Malformation Grade 8Document30 pagesNail Malformation Grade 8marbong coytopPas encore d'évaluation
- TLE CapsLet G10Document5 pagesTLE CapsLet G10Larnie De Ocampo PanalPas encore d'évaluation
- G-00-1169 - Grade Designation For Low Carbon Hot Rolled Steel Sheets Used in Automotive Applications - Rev 4Document7 pagesG-00-1169 - Grade Designation For Low Carbon Hot Rolled Steel Sheets Used in Automotive Applications - Rev 4Prince Ali50% (2)
- 1.4 BG00381946 - ADocument1 page1.4 BG00381946 - AAnand KesarkarPas encore d'évaluation
- Prototyping: by DR Sampa Unnikrishnan Yateer Creative Solutions Reachus@Yateer - In, 8971442777Document70 pagesPrototyping: by DR Sampa Unnikrishnan Yateer Creative Solutions Reachus@Yateer - In, 8971442777ShivashankarPas encore d'évaluation
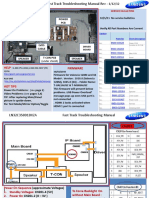
- Samsung LN55C610N1FXZA Fast Track Guide (SM)Document4 pagesSamsung LN55C610N1FXZA Fast Track Guide (SM)Carlos OdilonPas encore d'évaluation
- CV - en - Hamdaoui Mohamed AmineDocument2 pagesCV - en - Hamdaoui Mohamed AmineHAMDAOUI Mohamed Amine100% (1)
- Q4L6 Properties of KiteDocument8 pagesQ4L6 Properties of KiteAltheus Miguel Dela CruzPas encore d'évaluation
- Term Paper - 2022964Document17 pagesTerm Paper - 2022964Md. Ahbab HasanPas encore d'évaluation
- Net June 2013Document22 pagesNet June 2013Sunil PandeyPas encore d'évaluation
- PGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersDocument117 pagesPGT Computer Science Kendriya Vidyalaya Entrance Exam Question PapersimshwezPas encore d'évaluation
- Epri Guide For Transmission Line Groundingpdf PDF FreeDocument188 pagesEpri Guide For Transmission Line Groundingpdf PDF FreeHolman Wbeimar Suarez Niño100% (1)
- High Performance ComputingDocument294 pagesHigh Performance Computingsorinbazavan100% (1)
- Clay and Shale, Robert L VirtaDocument24 pagesClay and Shale, Robert L VirtaRifqi Brilyant AriefPas encore d'évaluation
- Sculpture and ArchitectureDocument9 pagesSculpture and ArchitectureIngrid Dianne Luga BernilPas encore d'évaluation
- Unit 2: TransducerDocument24 pagesUnit 2: TransducerROYAL GAMER YTPas encore d'évaluation
- DBL10 - Sapporo X Schematics Document: Compal ConfidentialDocument50 pagesDBL10 - Sapporo X Schematics Document: Compal ConfidentialEvgeniy BaranovskiyPas encore d'évaluation
- Content and Context Analysis of Selected Primary SourccesDocument3 pagesContent and Context Analysis of Selected Primary SourccesToshi CodmPas encore d'évaluation
- Pengaruh Pemberian Dosis Pupuk Urea Terhadap Pertumbuhan Tanaman Bayam Cabut Putih (AmaranthusDocument10 pagesPengaruh Pemberian Dosis Pupuk Urea Terhadap Pertumbuhan Tanaman Bayam Cabut Putih (AmaranthusMartha YhunickePas encore d'évaluation
- Jim 1000 RC 3Document33 pagesJim 1000 RC 3singingblueePas encore d'évaluation
- Historic Trial of Ali Brothers and Shankaracharya-1921Document276 pagesHistoric Trial of Ali Brothers and Shankaracharya-1921Sampath Bulusu100% (3)
- Working With Hierarchies External V08Document9 pagesWorking With Hierarchies External V08Devesh ChangoiwalaPas encore d'évaluation
- SFC PresentationDocument51 pagesSFC PresentationjmtriggerzPas encore d'évaluation
- Budgetary Quote HPE AMD 128cores For DNDSSGDocument7 pagesBudgetary Quote HPE AMD 128cores For DNDSSGglalit kumarPas encore d'évaluation
- E-Catalog 2021 Jan JMI Dan KimDocument52 pagesE-Catalog 2021 Jan JMI Dan KimbobPas encore d'évaluation
- Sheiko 13week Beginner ProgramDocument16 pagesSheiko 13week Beginner ProgramAnders DahlPas encore d'évaluation
- TSM 101 Course Outline (2022)Document2 pagesTSM 101 Course Outline (2022)ChryseanjPas encore d'évaluation
- Pengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahDocument13 pagesPengaruh Promosi Dan Brand Image (Citra Produk) Terhadap Loyalitas Pembelian Produk Pepsodent Di Ramayana Plaza, Jalan Aksara, Medan Dita AmanahAhmad HerdandiPas encore d'évaluation
- SIDPAC Standard Data Channels: Ch. No. Symbols Description UnitsDocument2 pagesSIDPAC Standard Data Channels: Ch. No. Symbols Description UnitsRGFEPas encore d'évaluation
- Artikel 8 - (CURRICULUM EVALUATION)Document12 pagesArtikel 8 - (CURRICULUM EVALUATION)Kikit8Pas encore d'évaluation