Vous aimerez peut-être aussi
- Introduction To BCCDocument36 pagesIntroduction To BCCachielariyoPas encore d'évaluation
- Creamer - An Introduction To Fully Integrated Mixed Methods Research PDFDocument289 pagesCreamer - An Introduction To Fully Integrated Mixed Methods Research PDFAngie Paola100% (2)
- The Theory of Planned Behaviour Reactions and ReflectionsDocument15 pagesThe Theory of Planned Behaviour Reactions and Reflectionsafca32Pas encore d'évaluation
- Ajzen's Theory of Planned Behavior and Social Media UseDocument20 pagesAjzen's Theory of Planned Behavior and Social Media UseWanRezawanaWanDaudPas encore d'évaluation
- The Effectiveness of Virtual Work To Keep Achieving Optimal Performance Amid The Covid-19 Virus OutbreakDocument5 pagesThe Effectiveness of Virtual Work To Keep Achieving Optimal Performance Amid The Covid-19 Virus OutbreakChristianWiradendiPas encore d'évaluation
- Ajzen, Icek. (1991) The Theory of Planned BehaviorDocument33 pagesAjzen, Icek. (1991) The Theory of Planned BehaviorrafaelfdhPas encore d'évaluation
- Organizational ClimateDocument3 pagesOrganizational ClimateSaba Nafees100% (1)
- Challenges of Middle and Late Adolescents BitchDocument8 pagesChallenges of Middle and Late Adolescents BitchBrielle PerezPas encore d'évaluation
- CBM Research ConceptualizationDocument14 pagesCBM Research Conceptualizationmark justine manutaPas encore d'évaluation
- Concept of Research ABKDocument48 pagesConcept of Research ABKAbdul Yahaya Dogonbaba100% (1)
- NURS - FPX 5005 - Brendan Madden - Assessment - 2-1Document9 pagesNURS - FPX 5005 - Brendan Madden - Assessment - 2-1SohaibPas encore d'évaluation
- Attention and ComprehensionDocument22 pagesAttention and ComprehensionAhmadd FadlyPas encore d'évaluation
- Theory of Planned BehaviorDocument2 pagesTheory of Planned Behaviorvespr33% (3)
- Unit 10 Group Behavior: Book Code MB 0022 (OB)Document35 pagesUnit 10 Group Behavior: Book Code MB 0022 (OB)Megha MathurPas encore d'évaluation
- Models of Organizational BehaviorDocument20 pagesModels of Organizational Behaviorlibroaklat100% (3)
- Tuckman Stages of Group Development: By: Aliska Muna Sagun and SapanDocument35 pagesTuckman Stages of Group Development: By: Aliska Muna Sagun and SapansagunPas encore d'évaluation
- Supply Chain Management For Higher EducationDocument15 pagesSupply Chain Management For Higher Educationprateekbapna90Pas encore d'évaluation
- QuantitativeDocument36 pagesQuantitativeMadhan MohanPas encore d'évaluation
- Mixed Method Research: An OverviewDocument16 pagesMixed Method Research: An Overviewshumon2657100% (1)
- Basics of The Decision MakingDocument4 pagesBasics of The Decision MakingStanly KimunyaPas encore d'évaluation
- 18 - Chapter 3 LeadershipDocument182 pages18 - Chapter 3 LeadershipBala MuruganPas encore d'évaluation
- Research MethodologyDocument28 pagesResearch MethodologyKhurshid A. KhanPas encore d'évaluation
- Theory of ChangeDocument10 pagesTheory of Changemais alyPas encore d'évaluation
- Theory of Reasoned ActionDocument8 pagesTheory of Reasoned ActionraulrajsharmaPas encore d'évaluation
- Export and Domestic SalesDocument17 pagesExport and Domestic SalesHenry DongPas encore d'évaluation
- Article Critique On Operation Management StudyDocument1 pageArticle Critique On Operation Management StudyValerie SintiPas encore d'évaluation
- Decision Making ModelDocument7 pagesDecision Making Modelcstraubel7507100% (1)
- Research Methods AssignmentDocument4 pagesResearch Methods AssignmentSadia JunaidPas encore d'évaluation
- Human Relations Approach To ManagementDocument1 pageHuman Relations Approach To ManagementArun SastryPas encore d'évaluation
- Difference Between Qualitative & Quantitative Methods As Used in Project M&EDocument12 pagesDifference Between Qualitative & Quantitative Methods As Used in Project M&EisaactibenkanaPas encore d'évaluation
- Critiques of Mixed Methods Research StudiesDocument18 pagesCritiques of Mixed Methods Research Studiesmysales100% (1)
- Philosophical FrameworksDocument9 pagesPhilosophical FrameworksmusharukwaPas encore d'évaluation
- Risk AssignmentDocument53 pagesRisk AssignmentNafiz ImtiazPas encore d'évaluation
- The Importance of Communication Skills in Negotiation An Empirical StudyDocument30 pagesThe Importance of Communication Skills in Negotiation An Empirical StudyPrabir Acharya100% (1)
- Theory of Planned BehaviorDocument6 pagesTheory of Planned BehaviorSeenauth Veeraj100% (1)
- Impacto de Influencers en La Decisiónde CompraDocument17 pagesImpacto de Influencers en La Decisiónde CompraYuleisi GonzalesPas encore d'évaluation
- TQM Barriers To TQM ImplementationDocument6 pagesTQM Barriers To TQM ImplementationShrutit21Pas encore d'évaluation
- MotivationDocument13 pagesMotivationFRANCIESPas encore d'évaluation
- Educational ResearchDocument77 pagesEducational ResearchTariq AhmadPas encore d'évaluation
- Mixed MethodsDocument1 pageMixed MethodsJM Jesalva BalanquitPas encore d'évaluation
- Int. J. Production Economics: Changiz Valmohammadi, Shervin RoshanzamirDocument12 pagesInt. J. Production Economics: Changiz Valmohammadi, Shervin RoshanzamirdheaPas encore d'évaluation
- Motivational TheoryDocument23 pagesMotivational TheoryAsad Khan100% (1)
- Mixed MethodDocument26 pagesMixed MethodFirdaus AzizPas encore d'évaluation
- Case Study SampleDocument5 pagesCase Study SampleNeri NeriPas encore d'évaluation
- APJ5Feb17 4247 1Document21 pagesAPJ5Feb17 4247 1Allan Angelo GarciaPas encore d'évaluation
- Difference Between Quantitative and Qualitative Research in The Perspective of The Research ParadigmDocument3 pagesDifference Between Quantitative and Qualitative Research in The Perspective of The Research ParadigmQamar Zaman MalikPas encore d'évaluation
- Chapter3 - Skills Approach To LeadershipDocument34 pagesChapter3 - Skills Approach To LeadershipMary Pauline Musca100% (2)
- Stakeholder Analysis - : Kelembagaan Dalam Perumahan Dan PermukimanDocument18 pagesStakeholder Analysis - : Kelembagaan Dalam Perumahan Dan Permukimansella guslandaPas encore d'évaluation
- Technology Acceptance Model PDFDocument10 pagesTechnology Acceptance Model PDFTitat Placedes TaniogPas encore d'évaluation
- Critical ReflectionDocument4 pagesCritical ReflectionMahalaleel QuilantangPas encore d'évaluation
- Chapter 1 History of ManagementDocument39 pagesChapter 1 History of ManagementCerise Pastel100% (1)
- Organizational Process Models of Decision MakingDocument2 pagesOrganizational Process Models of Decision MakingKhan AmirPas encore d'évaluation
- Final ProjectDocument14 pagesFinal ProjectShivangi VaidPas encore d'évaluation
- Using The Theory of Planned Behavior To Determine The Social Network Usage Behavior in Saudi ArabiaDocument9 pagesUsing The Theory of Planned Behavior To Determine The Social Network Usage Behavior in Saudi ArabiaWhite Globe Publications (IJORCS)Pas encore d'évaluation
- Organizational ConflictDocument16 pagesOrganizational ConflictpRiNcE DuDhAtRaPas encore d'évaluation
- Organizational Climate: BY: Ms Namita Arya Asst. Professor EconDocument40 pagesOrganizational Climate: BY: Ms Namita Arya Asst. Professor EconnamitaPas encore d'évaluation
- Theory of Planned BehaviorDocument2 pagesTheory of Planned BehaviorAngeloPas encore d'évaluation
- Social MKTG PPT 3Document17 pagesSocial MKTG PPT 3abdelamuzemil8Pas encore d'évaluation
- Theories and Models in AIDS PREVENTIONDocument14 pagesTheories and Models in AIDS PREVENTIONMatin Ahmad KhanPas encore d'évaluation
- Lesson Plan: Religion and Revenge in "Hamlet"Document2 pagesLesson Plan: Religion and Revenge in "Hamlet"kkalmes1992Pas encore d'évaluation
- TCS PassagesDocument91 pagesTCS PassagesRachanaPas encore d'évaluation
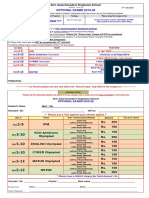
- Optional Exams 2019-20: Smt. Sulochanadevi Singhania SchoolDocument1 pageOptional Exams 2019-20: Smt. Sulochanadevi Singhania SchoolRamanand YadavPas encore d'évaluation
- ACI FormDocument1 pageACI FormToyosi OlugbenlePas encore d'évaluation
- Api111 Syllabus 0819Document6 pagesApi111 Syllabus 0819qaz333Pas encore d'évaluation
- 3p's GuideDocument14 pages3p's GuideElla CustodioPas encore d'évaluation
- DLP Cookery SAMPLEDocument9 pagesDLP Cookery SAMPLEMha Riz100% (4)
- System of Equations Lesson PlanDocument3 pagesSystem of Equations Lesson Planapi-489866539Pas encore d'évaluation
- Is College For Everyone - RevisedDocument5 pagesIs College For Everyone - Revisedapi-295480043Pas encore d'évaluation
- B.tech.-II 3rd Sem ChemicalDocument7 pagesB.tech.-II 3rd Sem Chemicalryan10rajPas encore d'évaluation
- New York Times War and Memory LessonDocument39 pagesNew York Times War and Memory Lessonapi-218930601Pas encore d'évaluation
- Monitoring and Evaluation of Online LearningDocument8 pagesMonitoring and Evaluation of Online LearningFadjar Eko NovantoPas encore d'évaluation
- Evaluation Rating Sheet For Non Print LR MaterialsDocument8 pagesEvaluation Rating Sheet For Non Print LR MaterialsMica BernabePas encore d'évaluation
- Chapter 12 PracticeDocument96 pagesChapter 12 PracticeDavid VundiPas encore d'évaluation
- E Importance of Studying RizalDocument2 pagesE Importance of Studying RizalBig_vain67% (3)
- The Doctrine of Forms Under Critique Part II - Metaphysics A 9Document27 pagesThe Doctrine of Forms Under Critique Part II - Metaphysics A 9blavskaPas encore d'évaluation
- Literacy Strategy Lesson Plan-Thought BubbleDocument5 pagesLiteracy Strategy Lesson Plan-Thought Bubbleapi-287993401Pas encore d'évaluation
- The Rizal Technological UniversityDocument3 pagesThe Rizal Technological UniversityHerald PadillaPas encore d'évaluation
- Carl Orff - Fortuna Imperatrix Mundi (Carmina Burana) - Arr. Wolfgang Vrecun PDFDocument4 pagesCarl Orff - Fortuna Imperatrix Mundi (Carmina Burana) - Arr. Wolfgang Vrecun PDFVMSPPas encore d'évaluation
- STES Edgardo Pacua May, 2021 Accomplishment ReportDocument5 pagesSTES Edgardo Pacua May, 2021 Accomplishment ReportDebz CayPas encore d'évaluation
- Cot English 8 Composing Effective ParagraphDocument5 pagesCot English 8 Composing Effective ParagraphJerwin Mojico100% (9)
- Powerpoint 2Document14 pagesPowerpoint 2api-406983345Pas encore d'évaluation
- Subclass 476 Skilled-Recognised Graduate VisaDocument18 pagesSubclass 476 Skilled-Recognised Graduate VisaFaisal Gulzar100% (1)
- Paper 3 Non Calc June 2010 Detailed SolutionsDocument24 pagesPaper 3 Non Calc June 2010 Detailed SolutionsNeil BradfordPas encore d'évaluation
- LWWR FinalsDocument23 pagesLWWR FinalsAndrea ElcanoPas encore d'évaluation
- Queen Mary University DissertationDocument5 pagesQueen Mary University DissertationWhereToBuyResumePaperLosAngeles100% (1)
- Gen Math GAS Daily Lesson LogDocument5 pagesGen Math GAS Daily Lesson Logjun del rosario100% (2)
- The Folklore of Language Teaching. Thomas F. Magner (1965)Document6 pagesThe Folklore of Language Teaching. Thomas F. Magner (1965)Turcology TiranaPas encore d'évaluation
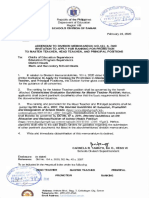
- Division Memo No 118, S.2020 - ADDENDUM TO DIVISION MEMO NO 109 S.2020 RE INVITATION TO APPLY FOR RANKING FOR PROMOTION TO MASTER TEACHER, HEAD TEACHER AND PRINCIPAL POSITIONSDocument5 pagesDivision Memo No 118, S.2020 - ADDENDUM TO DIVISION MEMO NO 109 S.2020 RE INVITATION TO APPLY FOR RANKING FOR PROMOTION TO MASTER TEACHER, HEAD TEACHER AND PRINCIPAL POSITIONSCristal Iba?zPas encore d'évaluation
- CAT 99%iler Club!: BtribeDocument4 pagesCAT 99%iler Club!: BtribeShivangi AgrawalPas encore d'évaluation