Vous aimerez peut-être aussi
- Bio-Mechanics MarkersDocument3 pagesBio-Mechanics MarkersMateus GalliPas encore d'évaluation
- Pulsed RF - Nikolai BogdukDocument12 pagesPulsed RF - Nikolai BogdukMateus GalliPas encore d'évaluation
- Graphing An Elliptic Paraboloid: Elliptical Cross-SectionDocument6 pagesGraphing An Elliptic Paraboloid: Elliptical Cross-SectionMateus GalliPas encore d'évaluation
- UntitledDocument1 pageUntitledMateus GalliPas encore d'évaluation
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Professional ResumeDocument1 pageProfessional ResumeDouglas RutledgePas encore d'évaluation
- Abdominal Pain Content PDFDocument71 pagesAbdominal Pain Content PDFyanPas encore d'évaluation
- Dosage Calc ReviewDocument24 pagesDosage Calc ReviewKara Dawn Mason100% (1)
- I. Mother and Child HealthDocument70 pagesI. Mother and Child Healthconahs nasugbuPas encore d'évaluation
- Infertility Social ImpactDocument3 pagesInfertility Social ImpactAlisha SyiemliehPas encore d'évaluation
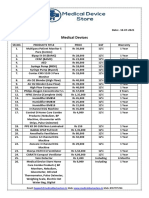
- Medical Device Store Products CatalogueDocument3 pagesMedical Device Store Products CatalogueWasim KhatibPas encore d'évaluation
- Class SelectionDocument6 pagesClass SelectionPhilip_830Pas encore d'évaluation
- Femur Fractures in Children - Case PresentationDocument22 pagesFemur Fractures in Children - Case PresentationChristian MicallefPas encore d'évaluation
- Health Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthDocument50 pagesHealth Facilities and Services Regulatory Bureau: Republic of The Philippines Department of HealthShu Dizon100% (1)
- Catalogue 2013-2014Document20 pagesCatalogue 2013-2014Ahmed DolaPas encore d'évaluation
- Enigma 1 Trial 2007Document11 pagesEnigma 1 Trial 2007Jason TiongPas encore d'évaluation
- History of Dental RadiologyDocument7 pagesHistory of Dental RadiologyAnu SushanthPas encore d'évaluation
- Sailing On The SS Serpa PintoDocument8 pagesSailing On The SS Serpa PintoFausto Gardini100% (1)
- Nursing Chart For All Nursing Boards 2010cllientDocument4 pagesNursing Chart For All Nursing Boards 2010cllientshooestPas encore d'évaluation
- Thoracic & Abdominal Wall BlocksDocument57 pagesThoracic & Abdominal Wall Blocksvignoth23112000Pas encore d'évaluation
- 03 The Role of "Smart" Infusion Pumps in Patient Safety PDFDocument11 pages03 The Role of "Smart" Infusion Pumps in Patient Safety PDFSaravanan NallasivanPas encore d'évaluation
- Partograph NotessssDocument17 pagesPartograph NotessssSunil KumarPas encore d'évaluation
- The Pros and Cons of Spaying A SheltieDocument15 pagesThe Pros and Cons of Spaying A SheltiepsykosomatikPas encore d'évaluation
- The Preoperative EvaluationDocument25 pagesThe Preoperative Evaluationnormie littlemonsterPas encore d'évaluation
- WHO:SURGICAL WORKFORCE IN INDIA-What The State of Kerala Tells Us About The Production, Stock and Migration of The Health WorkforceDocument33 pagesWHO:SURGICAL WORKFORCE IN INDIA-What The State of Kerala Tells Us About The Production, Stock and Migration of The Health Workforcemahwish khanPas encore d'évaluation
- Acute Abdomen FinalDocument105 pagesAcute Abdomen FinalAizul AzmiPas encore d'évaluation
- Prolapso de Cordón 1Document10 pagesProlapso de Cordón 1Jhonatan MendozaPas encore d'évaluation
- DT117 - Sem 1 - Week 17Document1 pageDT117 - Sem 1 - Week 17Kelly YeowPas encore d'évaluation
- Director Operations Demonstration Manager in Kansas City Resume Alex FitchDocument2 pagesDirector Operations Demonstration Manager in Kansas City Resume Alex FitchAlexFitch2Pas encore d'évaluation
- Nlex 1Document4 pagesNlex 1Aileen AlphaPas encore d'évaluation
- Er Medicine ReviewDocument16 pagesEr Medicine Reviewsdb10cPas encore d'évaluation
- A Study On Internal Fixation of Bimalleolar Ankle FracturesDocument4 pagesA Study On Internal Fixation of Bimalleolar Ankle FracturesIOSRjournalPas encore d'évaluation
- Anaesthesiology Case (Kaarthigan)Document36 pagesAnaesthesiology Case (Kaarthigan)Kaarthigan RamaiahPas encore d'évaluation
- O&G SyllabusDocument8 pagesO&G SyllabusHo Yong WaiPas encore d'évaluation
- Easa Caa Class 1Document2 pagesEasa Caa Class 1A0938746599273927Pas encore d'évaluation