Vous aimerez peut-être aussi
- Circulatory System OverviewDocument65 pagesCirculatory System OverviewgedesuryawanPas encore d'évaluation
- Vessels Nerves and Conducting System ofDocument55 pagesVessels Nerves and Conducting System ofHere LeafsPas encore d'évaluation
- 5 - Cardio, RespiDocument287 pages5 - Cardio, RespiBeth CuntapayPas encore d'évaluation
- Heart AnatomyDocument178 pagesHeart AnatomysubbuPas encore d'évaluation
- Royal Free Hospital Heart Attack Centre Admission ProcessDocument36 pagesRoyal Free Hospital Heart Attack Centre Admission Processb aPas encore d'évaluation
- Cardiac Imaging-AnatomyDocument27 pagesCardiac Imaging-AnatomyfatimaPas encore d'évaluation
- Clinical Cardiology Made Ridiculously Simple 4th Ed [Medicalstudyzone.com]Document388 pagesClinical Cardiology Made Ridiculously Simple 4th Ed [Medicalstudyzone.com]Fael BougdalPas encore d'évaluation
- 12 Lead Ecg or EkgDocument24 pages12 Lead Ecg or EkgSid KhanPas encore d'évaluation
- 1.basic HemoDocument64 pages1.basic HemoCathlab RS Soedarso PontianakPas encore d'évaluation
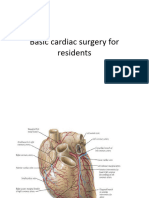
- Basic Cardiac Surgery For ResidentsDocument53 pagesBasic Cardiac Surgery For ResidentsIntrusive ReaderPas encore d'évaluation
- Anatomy of The Coronary Arteries and VeinsDocument80 pagesAnatomy of The Coronary Arteries and Veinstreelife111Pas encore d'évaluation
- Adi Bestara EKG at A Glance NewestDocument113 pagesAdi Bestara EKG at A Glance Newestkarpax21100% (1)
- B&B CVS - AnatomyDocument8 pagesB&B CVS - AnatomyMohammed HalimyPas encore d'évaluation
- Kuliah Radiologi Cardiorespiratory 2Document99 pagesKuliah Radiologi Cardiorespiratory 2Muhammad Sandy Ali YafiePas encore d'évaluation
- Cardiovascular System: Dr. Dipti VasaniDocument52 pagesCardiovascular System: Dr. Dipti Vasaniaarti HingePas encore d'évaluation
- 12 Lead EKG 101: A Guide to Interpreting EKGs and Treating Cardiac PatientsDocument84 pages12 Lead EKG 101: A Guide to Interpreting EKGs and Treating Cardiac Patientszul fatmah100% (1)
- Cardiovascular Assessment LectureDocument116 pagesCardiovascular Assessment LectureJohnryl FranciscoPas encore d'évaluation
- Circulatory SystemDocument43 pagesCirculatory SystemRestu DwikelanaPas encore d'évaluation
- Cardiac Imaging V03jul2012Document80 pagesCardiac Imaging V03jul2012nganklaiPas encore d'évaluation
- 12 Lead EKG 101Document84 pages12 Lead EKG 101Clarke KrugmanPas encore d'évaluation
- 01 HeartDocument39 pages01 HeartFahvy tvPas encore d'évaluation
- 5.4 Heart f2f-s1b2-23Document36 pages5.4 Heart f2f-s1b2-23shlokPas encore d'évaluation
- Cardiovascular Physiology: Anatomy and Functions of the HeartDocument42 pagesCardiovascular Physiology: Anatomy and Functions of the HeartancillaagraynPas encore d'évaluation
- 4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - SurgeryDocument60 pages4 - Toronto Notes 2011 - Cardiology - and - Cardiovascular - Surgeryqobsar100% (1)
- Medmastery Handbook ACHD 0Document127 pagesMedmastery Handbook ACHD 0Vladlena Cucoș-Caraiman100% (1)
- Cardiovascular Physiology by Dr. Sana Bashir MS-CPPT, DPTDocument42 pagesCardiovascular Physiology by Dr. Sana Bashir MS-CPPT, DPTbkdfiesefllPas encore d'évaluation
- Cardio NursingDocument141 pagesCardio NursingKhatlen BagaresPas encore d'évaluation
- ElectrocardiogramDocument52 pagesElectrocardiogramTuong HoangManhPas encore d'évaluation
- Cardiovascular SystemDocument11 pagesCardiovascular SystemРахым ХасеновPas encore d'évaluation
- Cardiovascular Anatomy and Physiology GuideDocument44 pagesCardiovascular Anatomy and Physiology GuidetoryPas encore d'évaluation
- Congenital Heart Diseases: Non Cyanotic PlethoraDocument43 pagesCongenital Heart Diseases: Non Cyanotic PlethoraFauzi SatriaPas encore d'évaluation
- Heart ImagesDocument74 pagesHeart ImagesNaveen EldosePas encore d'évaluation
- b4n - 1 - Basic Cvs Physiology & EcgDocument56 pagesb4n - 1 - Basic Cvs Physiology & EcgMerganey TebenPas encore d'évaluation
- The Cardiovascular System in ActionDocument28 pagesThe Cardiovascular System in ActionCharmen Evangelio Pabilona-FloresPas encore d'évaluation
- Anatomi Dan Fisiologi Jantung: RONI YULIWAR, S.Kep, NS, M.KedDocument72 pagesAnatomi Dan Fisiologi Jantung: RONI YULIWAR, S.Kep, NS, M.KedAnonymous Q4t8YxPas encore d'évaluation
- The Cardiovascular SystemDocument98 pagesThe Cardiovascular SystemTikboy TaliliPas encore d'évaluation
- Intrinsic Conducting System - CVS-K2 UmsuDocument44 pagesIntrinsic Conducting System - CVS-K2 Umsudwi ariskaPas encore d'évaluation
- Online Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreDocument87 pagesOnline Practice Tests, Live Classes, Tutoring, Study Guides Q&A, Premium Content and MoreYoAmoNYCPas encore d'évaluation
- IschemicHeartDisease LectureDocument64 pagesIschemicHeartDisease Lectureahmad usmanPas encore d'évaluation
- 19, Fetal Circulation& Heamo.. Congenital Heart DiseaseDocument59 pages19, Fetal Circulation& Heamo.. Congenital Heart Diseasesumayya hameedPas encore d'évaluation
- 1- Cardiac Anatomy ♫Document8 pages1- Cardiac Anatomy ♫jeannedarcachkarPas encore d'évaluation
- Cardiac and Coronary AnatomyDocument19 pagesCardiac and Coronary Anatomymeta ikaPas encore d'évaluation
- Heart Anatomy and Physiology PDFDocument100 pagesHeart Anatomy and Physiology PDFAndrés Menéndez Rojas100% (1)
- Cardiovascular System and Disorders (Original)Document36 pagesCardiovascular System and Disorders (Original)Wirya PratamaPas encore d'évaluation
- Intrinsic Conducting System ECGDocument43 pagesIntrinsic Conducting System ECGJane Andrea Christiano DjianzoniePas encore d'évaluation
- Imaging of the Heart: Radiographic Findings of Normal Anatomy and Common PathologiesDocument51 pagesImaging of the Heart: Radiographic Findings of Normal Anatomy and Common PathologiesadystiPas encore d'évaluation
- Cardiac SurgeryDocument110 pagesCardiac SurgeryChristopher McAndrew100% (1)
- Kasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHDocument34 pagesKasus 6 (ADHF Grade II + NSTEMI + HHD + Dislipidemia) - Blok CVS - Tingkat 2 - NRP 1910211099 - REZA RAMADHANSYAHReza RamadhansyahPas encore d'évaluation
- Cardiac Anatomy and Physiology: Leaugeay Webre BS, CCEMT-P, Nremt-PDocument145 pagesCardiac Anatomy and Physiology: Leaugeay Webre BS, CCEMT-P, Nremt-Pa.abdullah.2005.111Pas encore d'évaluation
- (K29) Electrocardiogram CVSDocument43 pages(K29) Electrocardiogram CVSXeniel AlastairPas encore d'évaluation
- پرستاری داخلی و جراحی قلب (Autosaved)Document70 pagesپرستاری داخلی و جراحی قلب (Autosaved)ayoub.panahi6716Pas encore d'évaluation
- Introduction To The Cardiopulmonary Systems: Lecture On Sept 6th & Sept 9thDocument30 pagesIntroduction To The Cardiopulmonary Systems: Lecture On Sept 6th & Sept 9thEngineers go fishing JustkiddingPas encore d'évaluation
- Lecture Notes on Anatomy and Physiology of the Cardiovascular SystemDocument18 pagesLecture Notes on Anatomy and Physiology of the Cardiovascular SystemLudwigJayBarayuga100% (5)
- Project HHC-EMT-P Training ProgramDocument33 pagesProject HHC-EMT-P Training ProgramPradeep KumarPas encore d'évaluation
- Applied Anatomy of The Heart - StudentDocument38 pagesApplied Anatomy of The Heart - StudentNatalia RomanPas encore d'évaluation
- Cardiovascular System Study SheetDocument8 pagesCardiovascular System Study SheetTkPas encore d'évaluation
- ANPATH1 Cardiovascular SystemDocument21 pagesANPATH1 Cardiovascular SystemYancy BagsaoPas encore d'évaluation
- Cardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariDocument42 pagesCardiac Anatomy, Physiology, and Cardiac Cycle: Ayu Puspita SariAyu PuspitaPas encore d'évaluation
- EKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationD'EverandEKG | ECG Interpretation. Everything You Need to Know about 12-Lead ECG/EKG InterpretationÉvaluation : 3 sur 5 étoiles3/5 (1)
- Premature (Early) Ejaculation, Delayed Ejaculation and ErectileDocument78 pagesPremature (Early) Ejaculation, Delayed Ejaculation and ErectileTemesgen EndalewPas encore d'évaluation
- DTS, RapeDocument73 pagesDTS, RapeTemesgen EndalewPas encore d'évaluation
- Dissociative Identity DisorderDocument66 pagesDissociative Identity DisorderTemesgen Endalew100% (1)
- Update: Diagnostic Statistical Manual Mental DisordersDocument30 pagesUpdate: Diagnostic Statistical Manual Mental DisordersTemesgen EndalewPas encore d'évaluation
- GerdQ self-assessment questionnaire appendixDocument1 pageGerdQ self-assessment questionnaire appendixTemesgen EndalewPas encore d'évaluation
- Clozapine Is EverywhereDocument1 pageClozapine Is EverywhereTemesgen EndalewPas encore d'évaluation
- Principles and Techniques of Oral BiopsyDocument45 pagesPrinciples and Techniques of Oral BiopsyMahamoud IsmailPas encore d'évaluation
- Who Mental Health Report PDFDocument10 pagesWho Mental Health Report PDFTemesgen EndalewPas encore d'évaluation
- Mental Illness Is Nothing To Be Ashamed ofDocument5 pagesMental Illness Is Nothing To Be Ashamed ofTemesgen EndalewPas encore d'évaluation
- List of Books: S.N Author Title Publication ISBN QTY RemarkDocument2 pagesList of Books: S.N Author Title Publication ISBN QTY RemarkTemesgen EndalewPas encore d'évaluation
- Overview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyDocument3 pagesOverview: Mechanisms of Hypertension: Cells, Hormones, and The KidneyTemesgen EndalewPas encore d'évaluation
- To My Facebook WallDocument1 pageTo My Facebook WallTemesgen EndalewPas encore d'évaluation
- Oral Health Complications and HIV-Infected PatientsDocument14 pagesOral Health Complications and HIV-Infected PatientsTemesgen EndalewPas encore d'évaluation
- Excise Tax Proclamation No 307 2002Document22 pagesExcise Tax Proclamation No 307 2002Temesgen EndalewPas encore d'évaluation
- GynObs Outline For QualifiersDocument5 pagesGynObs Outline For QualifiersTemesgen EndalewPas encore d'évaluation
- EDs Basic Histology PDFDocument208 pagesEDs Basic Histology PDFTemesgen Endalew0% (1)
- Entrance Exam: September 2022Document2 pagesEntrance Exam: September 2022Temesgen EndalewPas encore d'évaluation
- Generic Project Proposal TemplateDocument9 pagesGeneric Project Proposal TemplateTemesgen EndalewPas encore d'évaluation
- Recommended Texts / Useful Resources For Psychiatry TraineesDocument5 pagesRecommended Texts / Useful Resources For Psychiatry TraineesTemesgen EndalewPas encore d'évaluation
- How To Read A Systematic Review and Meta-Analysis and Apply The Results To Patient CareDocument9 pagesHow To Read A Systematic Review and Meta-Analysis and Apply The Results To Patient CareTemesgen EndalewPas encore d'évaluation
- Hemodynamic DysorderDocument158 pagesHemodynamic DysorderTemesgen EndalewPas encore d'évaluation
- Learning For Performance: A Guide and Toolkit For Health Worker Training and Education ProgramsDocument84 pagesLearning For Performance: A Guide and Toolkit For Health Worker Training and Education ProgramsTemesgen EndalewPas encore d'évaluation
- World Health Organization Classification of TumourDocument42 pagesWorld Health Organization Classification of TumourTemesgen EndalewPas encore d'évaluation
- The Love DareDocument4 pagesThe Love DareJeffrey Portalanza100% (3)
- InflammationDocument81 pagesInflammationTemesgen EndalewPas encore d'évaluation
- Abstract of ResearchDocument1 pageAbstract of ResearchTemesgen EndalewPas encore d'évaluation
- Proc No. 307-2002 Excise Tax PDFDocument15 pagesProc No. 307-2002 Excise Tax PDFTemesgen Endalew0% (1)
- Rligion Health and MedicieneDocument13 pagesRligion Health and MedicieneTemesgen EndalewPas encore d'évaluation
- Who Mental Health Report PDFDocument10 pagesWho Mental Health Report PDFTemesgen EndalewPas encore d'évaluation
- The ABCs of Heart Disease William HerringDocument14 pagesThe ABCs of Heart Disease William HerringHerchell Sayo SantosPas encore d'évaluation
- ENT-Laryngeal ParalysisDocument26 pagesENT-Laryngeal ParalysisRahul Kumar DiwakarPas encore d'évaluation
- Atlas of Intraoperative Transesophageal EchocardiographyDocument416 pagesAtlas of Intraoperative Transesophageal EchocardiographyDelia Acsinte100% (1)
- Transcatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsDocument22 pagesTranscatheter Tricuspid Valve Interventions: Landscape, Challenges, and Future DirectionsgPas encore d'évaluation
- Ecg MDDocument121 pagesEcg MDdr. snehal patilPas encore d'évaluation
- ABSTRACT TEVAR - Achmad Ismail S Putra NewDocument3 pagesABSTRACT TEVAR - Achmad Ismail S Putra NewPutra AchmadPas encore d'évaluation
- Cardiac CycleDocument14 pagesCardiac Cycleareznik3007Pas encore d'évaluation
- Detecting Heartbeats and Diagnosing Chest PainDocument113 pagesDetecting Heartbeats and Diagnosing Chest PainNasan Shehada100% (1)
- Left Ventricle To Left Atrial Fistula Caused by Perforated Perivalvular AbscessDocument2 pagesLeft Ventricle To Left Atrial Fistula Caused by Perforated Perivalvular AbscessAlznoskillPas encore d'évaluation
- Ic Interactive Product Catalogue Uk 2017Document83 pagesIc Interactive Product Catalogue Uk 2017RABAH BOUCHELAGHEMPas encore d'évaluation
- Thoracic 53Document53 pagesThoracic 53RaMy “MhMd” ElaRabyPas encore d'évaluation
- Cazuri-ColoanapptDocument69 pagesCazuri-ColoanapptmiravoineaPas encore d'évaluation
- Acynotic Congenital Heart Diseases: FFU May 2020Document14 pagesAcynotic Congenital Heart Diseases: FFU May 2020gibreilPas encore d'évaluation
- Manual Muscle Test of Cervical SpineDocument4 pagesManual Muscle Test of Cervical SpineDr Ahmed NabilPas encore d'évaluation
- Surface Anatomy of HeartDocument12 pagesSurface Anatomy of Heartramesh5889Pas encore d'évaluation
- Discussion RsovDocument30 pagesDiscussion RsovwarholeblackPas encore d'évaluation
- Cardiac Imaging CasesDocument278 pagesCardiac Imaging Casesandrew100% (1)
- DEFIB PPT at PrakaraDocument52 pagesDEFIB PPT at Prakarakvl kandulaPas encore d'évaluation
- Review Notes On The Anatomy of The LungDocument5 pagesReview Notes On The Anatomy of The LungNabil Abd El-tawabPas encore d'évaluation
- Cardiology Teaching PackageDocument9 pagesCardiology Teaching PackageRicy SaitePas encore d'évaluation
- Cardiac Imaging Sept 2016tDocument254 pagesCardiac Imaging Sept 2016tColeen Joyce NeyraPas encore d'évaluation
- Thoracic Injuries Nis 2022Document24 pagesThoracic Injuries Nis 2022StefanPas encore d'évaluation
- CH 9 Ribs SternumDocument105 pagesCH 9 Ribs SternumchrissPas encore d'évaluation
- Chir12006 Week 7 Study Guide Answers 1 3Document8 pagesChir12006 Week 7 Study Guide Answers 1 3api-469904011Pas encore d'évaluation
- MurmursDocument5 pagesMurmursAlexander G. Álvarez RojasPas encore d'évaluation
- Major Bones and Bone Groups: Skeletal SystemDocument4 pagesMajor Bones and Bone Groups: Skeletal Systemtupe salcedoPas encore d'évaluation
- Mitral StenosisDocument12 pagesMitral StenosisFasihi Junior0% (1)
- Chapter 24 - Alterations of Cardiovascular Function in Children - Nursing Test BanksDocument19 pagesChapter 24 - Alterations of Cardiovascular Function in Children - Nursing Test BanksNeLPas encore d'évaluation
- SonoAce - R7 - Reference Manual - EDocument231 pagesSonoAce - R7 - Reference Manual - Edailene silvaPas encore d'évaluation
- Assessing the Chest and AbdomenDocument19 pagesAssessing the Chest and AbdomenNicole BertulfoPas encore d'évaluation






![Clinical Cardiology Made Ridiculously Simple 4th Ed [Medicalstudyzone.com]](https://imgv2-1-f.scribdassets.com/img/document/720630535/149x198/928d3d3d19/1712423639?v=1)