Vous aimerez peut-être aussi
- Queueing TheoryDocument6 pagesQueueing TheoryElmer BabaloPas encore d'évaluation
- Business Ethics: 3 Semester MBADocument34 pagesBusiness Ethics: 3 Semester MBAsweet19girlPas encore d'évaluation
- Inventory costs breakdown for optimal planningDocument5 pagesInventory costs breakdown for optimal planningsaquib0863Pas encore d'évaluation
- PLANT LOCATION FACTORSDocument6 pagesPLANT LOCATION FACTORSPandu SrujanPas encore d'évaluation
- Selection ProcessDocument18 pagesSelection Process255820Pas encore d'évaluation
- Development of The Information SystemDocument2 pagesDevelopment of The Information Systemapi-260129366Pas encore d'évaluation
- Expected Utility Theory EssayDocument2 pagesExpected Utility Theory EssayKand HroppaPas encore d'évaluation
- 1.1 Management Information Systems: 1.1.1 CONCEPTDocument24 pages1.1 Management Information Systems: 1.1.1 CONCEPTSandip PudasainiPas encore d'évaluation
- Defination of Total Quality ManagementDocument4 pagesDefination of Total Quality ManagementAinnur ArifahPas encore d'évaluation
- Oral PresentationDocument6 pagesOral Presentationfaint101100% (1)
- Prof. Joy V. Lorin-Picar Davao Del Norte State College: New Visayas, Panabo CityDocument91 pagesProf. Joy V. Lorin-Picar Davao Del Norte State College: New Visayas, Panabo CityJeLo ReaNdelarPas encore d'évaluation
- Types of Simulation Models from Behavioral to Transistor LevelDocument2 pagesTypes of Simulation Models from Behavioral to Transistor LevelRudelsa Agcolicol LangamanPas encore d'évaluation
- Four Perspectives on Learning Theories in 40 CharactersDocument4 pagesFour Perspectives on Learning Theories in 40 CharactersAnsam LeePas encore d'évaluation
- Inside Stakeholders Are People Who Are Closest To An Organization andDocument4 pagesInside Stakeholders Are People Who Are Closest To An Organization andArshad MohdPas encore d'évaluation
- Types of SimulationDocument7 pagesTypes of SimulationMani KandanPas encore d'évaluation
- Limitations and Conclusion IntroDocument3 pagesLimitations and Conclusion Intropasign inPas encore d'évaluation
- Group NormsDocument3 pagesGroup NormssaimoomagainPas encore d'évaluation
- Principles of Business CommunicationDocument3 pagesPrinciples of Business Communicationapi-224920675Pas encore d'évaluation
- 1 What Is Portfolio Performance EvaluationDocument17 pages1 What Is Portfolio Performance EvaluationDarshan GadaPas encore d'évaluation
- The 10 Golden Rules of Effective ManagementDocument7 pagesThe 10 Golden Rules of Effective ManagementMay-Ann S. CahiligPas encore d'évaluation
- Measurement ScalesDocument6 pagesMeasurement ScalesRohit PandeyPas encore d'évaluation
- Labour Management RelationsDocument2 pagesLabour Management RelationsiitebaPas encore d'évaluation
- Critical Value in HematologyDocument8 pagesCritical Value in HematologySTARK DIAGNOSTICSPas encore d'évaluation
- Forces of ChangeDocument21 pagesForces of Changemwendaki100% (1)
- Benefits of InsuranceDocument42 pagesBenefits of InsurancerocksonPas encore d'évaluation
- Guide 6 basic toolsDocument30 pagesGuide 6 basic toolsdrs_mdu48Pas encore d'évaluation
- Cost EffectivenessDocument8 pagesCost EffectivenessMehul LakhaniPas encore d'évaluation
- Methods of Time SeriesDocument4 pagesMethods of Time SeriesDharmendra SPas encore d'évaluation
- Trend AnalysisDocument6 pagesTrend AnalysisJayden Duc TranPas encore d'évaluation
- Total Quality ManagementDocument2 pagesTotal Quality Managementkaushikbose81Pas encore d'évaluation
- Performance Appraisal InterviewDocument19 pagesPerformance Appraisal InterviewPrakash ParidaPas encore d'évaluation
- Arbitrage Pricing TheoryDocument4 pagesArbitrage Pricing TheoryVijaya KadiyalaPas encore d'évaluation
- EMH AssignmentDocument8 pagesEMH AssignmentJonathanPas encore d'évaluation
- Measures of Central Tendency and VariationDocument32 pagesMeasures of Central Tendency and VariationasratPas encore d'évaluation
- Lab Math Lec (Prelims)Document7 pagesLab Math Lec (Prelims)Merra VenzuelaPas encore d'évaluation
- IH Hospital Wide QI Master Spreadsheet 2023Document115 pagesIH Hospital Wide QI Master Spreadsheet 2023Uranchimeg MyagmarchimedPas encore d'évaluation
- Group NormsDocument13 pagesGroup NormsAnushriAdarshRathiPas encore d'évaluation
- Notes of Managerial EconomicsDocument24 pagesNotes of Managerial EconomicsJaved HussainPas encore d'évaluation
- CLIAbrochure8 PDFDocument12 pagesCLIAbrochure8 PDFAlexandr Chuvakov100% (1)
- Elements of TQM: Management Commitment, Customer FocusDocument3 pagesElements of TQM: Management Commitment, Customer FocusAti ZulkifliPas encore d'évaluation
- CAP Presentation On StatisticDocument88 pagesCAP Presentation On StatisticAmirul AriffPas encore d'évaluation
- Assignment On Intranet and ExtranetDocument2 pagesAssignment On Intranet and ExtranetNitin Verma100% (7)
- Overview of Research ProcessDocument3 pagesOverview of Research ProcessKenneth GuingabPas encore d'évaluation
- Lab Investigation of AnaemiasDocument109 pagesLab Investigation of AnaemiasMadhura ShekatkarPas encore d'évaluation
- Fmea in Organ TransplantDocument8 pagesFmea in Organ TransplantVinay GargPas encore d'évaluation
- Risk Management in The Medical Laboratory: Reducing Risk Through Application of StandardsDocument53 pagesRisk Management in The Medical Laboratory: Reducing Risk Through Application of Standardsfysi mack100% (2)
- Workload Indicators (Staffing Norms)Document131 pagesWorkload Indicators (Staffing Norms)asimsiPas encore d'évaluation
- What Is Fundamental AnalysisDocument13 pagesWhat Is Fundamental AnalysisvishnucnkPas encore d'évaluation
- Research Designs & MethodologiesDocument6 pagesResearch Designs & MethodologiesKumiqinPas encore d'évaluation
- Problems and Prospects of Marketing in Developing EconomiesDocument10 pagesProblems and Prospects of Marketing in Developing EconomiesSesha TeegalaPas encore d'évaluation
- Stock Market EfficiencyDocument31 pagesStock Market EfficiencySathish Kumar100% (1)
- Unit-Iv 1. Testing of HypothesisDocument28 pagesUnit-Iv 1. Testing of Hypothesismalleda haneeshPas encore d'évaluation
- Clinical Chemistry Methods Guide 2010: For Labquality Data ProcessingDocument103 pagesClinical Chemistry Methods Guide 2010: For Labquality Data Processingcamilovivi100% (1)
- Current Databases On Biological Variation: Pros, Cons and ProgressDocument10 pagesCurrent Databases On Biological Variation: Pros, Cons and ProgressCarlos PardoPas encore d'évaluation
- Normative and Descriptive Decision TheoryDocument4 pagesNormative and Descriptive Decision TheorySubodh SaharanPas encore d'évaluation
- Sop-Clinical PathologyDocument25 pagesSop-Clinical PathologyAniruddha Chatterjee100% (1)
- Corporate GovernanceDocument7 pagesCorporate GovernancePraveen CaesarPas encore d'évaluation
- Desirable Biological Variation Database Specifications - WestgardDocument10 pagesDesirable Biological Variation Database Specifications - WestgardElmyLiantika MaranantanPas encore d'évaluation
- 1010 - Analytical Data - Interpretation and TreatmentDocument16 pages1010 - Analytical Data - Interpretation and TreatmentAnonymous ulcdZToPas encore d'évaluation
- A Model For Reducing Medical ErrorsDocument4 pagesA Model For Reducing Medical ErrorsPinto PintoPas encore d'évaluation
- A Practical Guide For Public Health Laboratory Leaders 2006Document43 pagesA Practical Guide For Public Health Laboratory Leaders 2006msabryPas encore d'évaluation
- A Practical Guide For Public Health Laboratory Leaders 2006Document43 pagesA Practical Guide For Public Health Laboratory Leaders 2006msabryPas encore d'évaluation
- 014 Burd PDFDocument38 pages014 Burd PDFmsabryPas encore d'évaluation
- Biological Variation, A Practical Review, DR C. Ricos PDFDocument40 pagesBiological Variation, A Practical Review, DR C. Ricos PDFmsabryPas encore d'évaluation
- Biological Variation, A Practical Review, DR C. Ricos PDFDocument40 pagesBiological Variation, A Practical Review, DR C. Ricos PDFmsabryPas encore d'évaluation
- Ebook On How To Implement An AS9100Document61 pagesEbook On How To Implement An AS9100Abd Zouhier100% (1)
- WSHP Competency MapDocument4 pagesWSHP Competency MaptatonyPas encore d'évaluation
- QuestionDocument17 pagesQuestionlinga2014Pas encore d'évaluation
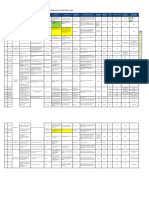
- BM TRADA ISO 9001 Correlation MatrixDocument10 pagesBM TRADA ISO 9001 Correlation MatrixArfan SaniPas encore d'évaluation
- TR-Pharmacy Services NC IIIDocument136 pagesTR-Pharmacy Services NC IIIAre Pee Etc100% (2)
- Revision Record Sheet: TitleDocument4 pagesRevision Record Sheet: TitleSanjay MalhotraPas encore d'évaluation
- ISO 9001 Training MaterialDocument248 pagesISO 9001 Training MaterialBuddharaju Kiran100% (2)
- Mandatory Documents IATF 16949Document10 pagesMandatory Documents IATF 16949Jm Venki100% (10)
- BSI ISO IEC 27001 Transition GuideDocument16 pagesBSI ISO IEC 27001 Transition GuideAlvaro Rodrigo Cayul0% (1)
- 8D Corrective Action Root CauseDocument95 pages8D Corrective Action Root Causealexrferreira100% (3)
- 8D Corrective Action & Root Cause AnalysisDocument95 pages8D Corrective Action & Root Cause AnalysisRawendrraw KuriPas encore d'évaluation
- HSE-P-08 Corrective and Preventive Action Issue 2.1Document5 pagesHSE-P-08 Corrective and Preventive Action Issue 2.1eng20072007Pas encore d'évaluation
- Corrective / Preventive Action ProcedureDocument3 pagesCorrective / Preventive Action ProcedureLovePas encore d'évaluation
- Food Safety Assurance SystemsDocument10 pagesFood Safety Assurance SystemsHiếu NguyễnPas encore d'évaluation
- NQA ISO 14001-2015 Transition Guidance PDFDocument6 pagesNQA ISO 14001-2015 Transition Guidance PDFMuhammad Saqib AsifPas encore d'évaluation
- Preventative Action Checklist: Steps StrategiesDocument2 pagesPreventative Action Checklist: Steps StrategiesBAlaPas encore d'évaluation
- BM TRADA ISO 9001 Overview Document PDFDocument15 pagesBM TRADA ISO 9001 Overview Document PDFNader ShdeedPas encore d'évaluation
- ICAO Safety RecommendationsDocument7 pagesICAO Safety RecommendationsSigit SasonoPas encore d'évaluation
- Checklist of OHSAS 18001 Mandatory Documentation enDocument8 pagesChecklist of OHSAS 18001 Mandatory Documentation enMiguelGarcés100% (1)
- 1 ISO 9001 - 2015 Overview OL TrainingDocument48 pages1 ISO 9001 - 2015 Overview OL TrainingTan Tok Hoi100% (1)
- C MR 01 02 Ims Check ListDocument16 pagesC MR 01 02 Ims Check ListShaileshPas encore d'évaluation
- WHO - TRS - 996 - Annex05 Guidance On Good Data and Record Management PracticesDocument46 pagesWHO - TRS - 996 - Annex05 Guidance On Good Data and Record Management PracticesAlfonso ZavaletaPas encore d'évaluation
- Stanley Business System EHS Road Map Management SystemDocument9 pagesStanley Business System EHS Road Map Management Systemjhun1203Pas encore d'évaluation
- ProjectDocument11 pagesProjectusman_usaf100% (1)
- ICH Q10 Pharmaceutical Quality System Apr12Document8 pagesICH Q10 Pharmaceutical Quality System Apr12geeenaaPas encore d'évaluation
- Product & Process Risk Assessment in Garments IndustryDocument5 pagesProduct & Process Risk Assessment in Garments IndustryMd SunnyPas encore d'évaluation
- 2015 ISO World Conference BrochureDocument50 pages2015 ISO World Conference BrochureAnonymous AlhzFE9EVNPas encore d'évaluation
- ISO 9001:2008 - Clause 4: 4.1 General RequirementsDocument14 pagesISO 9001:2008 - Clause 4: 4.1 General RequirementsRaajha MunibathiranPas encore d'évaluation
- KEBS ... ISO 9001-2015 Transition Guide (Secure)Document11 pagesKEBS ... ISO 9001-2015 Transition Guide (Secure)Venkatesan KattappanPas encore d'évaluation
- ISO 9001correlation MatricesDocument9 pagesISO 9001correlation Matricesrgopinath3102Pas encore d'évaluation