Vous aimerez peut-être aussi
- Aniteye 2013Document14 pagesAniteye 2013Mensah AdolphPas encore d'évaluation
- Shraddha ProjectDocument8 pagesShraddha ProjectshraddhagandhiPas encore d'évaluation
- Tech Brief Afghanistan FinalDocument5 pagesTech Brief Afghanistan FinalCharisse Diane MoradaPas encore d'évaluation
- Addressing Socio-Cultural Barriers To Maternal Healthcare in Ghana: Perspectives of Women and Healthcare ProvidersDocument11 pagesAddressing Socio-Cultural Barriers To Maternal Healthcare in Ghana: Perspectives of Women and Healthcare ProvidersEndah SuprihatinPas encore d'évaluation
- Telehealth Leaders' Attitudes Toward Telemedicine Provision of Medication Abortion: A Qualitative StudyDocument10 pagesTelehealth Leaders' Attitudes Toward Telemedicine Provision of Medication Abortion: A Qualitative StudymichyanggunPas encore d'évaluation
- Sexual & Reproductive Healthcare: SciencedirectDocument6 pagesSexual & Reproductive Healthcare: SciencedirectdeaPas encore d'évaluation
- TeleDocument9 pagesTeleElita RahmaPas encore d'évaluation
- Womens-Brochure 1025-004 508Document2 pagesWomens-Brochure 1025-004 508eeePas encore d'évaluation
- Assessment of Service Availability and Health CareDocument13 pagesAssessment of Service Availability and Health CareAbigail LausPas encore d'évaluation
- Post-Abortion Care in North Sulawesi, Indonesia Patients Determinants in Selection of Health FacilityDocument8 pagesPost-Abortion Care in North Sulawesi, Indonesia Patients Determinants in Selection of Health FacilityNununkPas encore d'évaluation
- Reproductive Health-Family Planning in Basrah - Evaluation of The Knowledge Utilization and Satisfaction of The Service UsersDocument11 pagesReproductive Health-Family Planning in Basrah - Evaluation of The Knowledge Utilization and Satisfaction of The Service UsersRajaa A. MahmoudPas encore d'évaluation
- Putting Abortion Pills Into Women's Hands: Realizing The Full Potential of Medical AbortionDocument4 pagesPutting Abortion Pills Into Women's Hands: Realizing The Full Potential of Medical AbortionFake_Me_Pas encore d'évaluation
- The Incidence of Induced Abortion in The PhilippinDocument11 pagesThe Incidence of Induced Abortion in The PhilippinJayram JavierPas encore d'évaluation
- Journal Pmed 1002341Document16 pagesJournal Pmed 1002341MaryPas encore d'évaluation
- Art 8Document27 pagesArt 8Jorge JosaphatPas encore d'évaluation
- Barriers To Immediate Post-Partum Intra-Uterine CoDocument14 pagesBarriers To Immediate Post-Partum Intra-Uterine CoConsolata kirigiaPas encore d'évaluation
- Does Antenatal Care Make A Difference To Safe Delivery? A Study in Urban Uttar Pradesh, IndiaDocument11 pagesDoes Antenatal Care Make A Difference To Safe Delivery? A Study in Urban Uttar Pradesh, IndiaLia Mbag LiaPas encore d'évaluation
- Improving The Implementation of Evidence Based Clinical P - 2015 - Journal of AdDocument8 pagesImproving The Implementation of Evidence Based Clinical P - 2015 - Journal of AdVahlufi Eka putriPas encore d'évaluation
- AbortionDocument1 pageAbortionVenus PlanetPas encore d'évaluation
- Women's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaDocument6 pagesWomen's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaakindunnidanielPas encore d'évaluation
- The Mistreatment of Women During, Bohren 2015Document32 pagesThe Mistreatment of Women During, Bohren 2015Umratun Sirajuddin AhmadPas encore d'évaluation
- Research Chapters 1 3Document19 pagesResearch Chapters 1 3mothballs2003Pas encore d'évaluation
- MLS 053 Group 10 Artificial Birth Control Case Study B8 FINALDocument15 pagesMLS 053 Group 10 Artificial Birth Control Case Study B8 FINALFrancine UriartePas encore d'évaluation
- 2020 Article 5726Document14 pages2020 Article 5726Khofifah IntanPas encore d'évaluation
- Preferences For A Potential Longer-Acting Injectable Contraceptive: Perspectives From Women, Providers, and Policy Makers in Kenya and RwandaDocument14 pagesPreferences For A Potential Longer-Acting Injectable Contraceptive: Perspectives From Women, Providers, and Policy Makers in Kenya and RwandaAbigail LausPas encore d'évaluation
- Essential Elements of Pac Model NotesDocument4 pagesEssential Elements of Pac Model NotesJoy KirumbaPas encore d'évaluation
- 1 Introduction - The Safety and Quality of Abortion Care in The United Sta172248Document20 pages1 Introduction - The Safety and Quality of Abortion Care in The United Sta172248Khrisha faith TayoPas encore d'évaluation
- Women's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaDocument6 pagesWomen's Perception of Antenatal Care Services in Public and Private Clinics in The GambiaNi Putu Yuni WidiasihPas encore d'évaluation
- Obstetric Violence For Professionals Who Assist in ChildbirthDocument9 pagesObstetric Violence For Professionals Who Assist in ChildbirthBetsy Mirella Ramirez PrietoPas encore d'évaluation
- s41182 023 00531 XDocument12 pagess41182 023 00531 Xmanage logPas encore d'évaluation
- Male Involvement and Maternal Health Outcomes: Systematic Review and Meta-AnalysisDocument9 pagesMale Involvement and Maternal Health Outcomes: Systematic Review and Meta-AnalysisRirinPakayaPas encore d'évaluation
- A Critical Overview of Abortion in IndiaDocument15 pagesA Critical Overview of Abortion in IndiaAnta SharmaPas encore d'évaluation
- Sterilisasi DilematisDocument14 pagesSterilisasi DilematisariniPas encore d'évaluation
- Disrespect and Abuse of Women During Childbirth in Nigeria: A Systematic ReviewDocument17 pagesDisrespect and Abuse of Women During Childbirth in Nigeria: A Systematic ReviewMaryPas encore d'évaluation
- Sexual & Reproductive Healthcare: EditorialDocument2 pagesSexual & Reproductive Healthcare: Editorialardian jayakusumaPas encore d'évaluation
- Contraception 2012 08 012Document22 pagesContraception 2012 08 012AjiPatriajatiPas encore d'évaluation
- Preconception Health and Care: A Life Course ApproachD'EverandPreconception Health and Care: A Life Course ApproachJill ShawePas encore d'évaluation
- Notes From The Field - Political Norm Change For Abortion in Pakistan - Taylor & Francis 2019Document8 pagesNotes From The Field - Political Norm Change For Abortion in Pakistan - Taylor & Francis 2019waqas724Pas encore d'évaluation
- Status of National Policy On Companion of Choice at Birth in Latin America and The Caribbean: Gaps and ChallengesDocument6 pagesStatus of National Policy On Companion of Choice at Birth in Latin America and The Caribbean: Gaps and ChallengesromaPas encore d'évaluation
- Faktor Askeb KomplementerDocument8 pagesFaktor Askeb KomplementerKadek Sri RahayuPas encore d'évaluation
- Research Gaps in The Care of Women With Female Genital Mutilation: An AnalysisDocument10 pagesResearch Gaps in The Care of Women With Female Genital Mutilation: An AnalysisHandaru KusumaPas encore d'évaluation
- Foster2018 PDFDocument1 pageFoster2018 PDFFake_Me_Pas encore d'évaluation
- Engaging Men in Maternal Health Strategies and Outcomes From Fort Portal Regional Referral Hospital, UgandaDocument15 pagesEngaging Men in Maternal Health Strategies and Outcomes From Fort Portal Regional Referral Hospital, UgandaKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Czac094Document11 pagesCzac094indahrizkygPas encore d'évaluation
- Factors in Uencing The Performance of Reproductive Health Care Service Providers in BasrahDocument11 pagesFactors in Uencing The Performance of Reproductive Health Care Service Providers in BasrahRajaa A. MahmoudPas encore d'évaluation
- Reproductive Health Services in PakistanDocument14 pagesReproductive Health Services in PakistanAli FaizanPas encore d'évaluation
- Kohn 2019Document8 pagesKohn 2019Elita RahmaPas encore d'évaluation
- Redesigning Primary Care Practice To Incorporate Health Behavior ChangeDocument3 pagesRedesigning Primary Care Practice To Incorporate Health Behavior ChangeDebbie CharlottePas encore d'évaluation
- Analysis of A UDocument6 pagesAnalysis of A Uapi-520453750Pas encore d'évaluation
- Refrence Article 1Document29 pagesRefrence Article 1Muhammad naveedPas encore d'évaluation
- Healthcare Policy Plan Nur420Document5 pagesHealthcare Policy Plan Nur420api-593188094Pas encore d'évaluation
- Assessment of Factors That Affect Male Partner Involvement in Emergency Obstetric Care in Fortportal Regional Referral HospitalDocument16 pagesAssessment of Factors That Affect Male Partner Involvement in Emergency Obstetric Care in Fortportal Regional Referral HospitalKIU PUBLICATION AND EXTENSIONPas encore d'évaluation
- Use of Evidence-Based Practices in Pregnancy and Childbirth: South East Asia Optimizing Reproductive and Child Health in Developing Countries ProjectDocument4 pagesUse of Evidence-Based Practices in Pregnancy and Childbirth: South East Asia Optimizing Reproductive and Child Health in Developing Countries ProjectZoe Jisel LuzadasPas encore d'évaluation
- Abortion Project FindingsDocument9 pagesAbortion Project FindingsuhhmbikaPas encore d'évaluation
- 14 KnowledgeofContraceptivesMethodsandAppraisalofHealthEducationamongMarriedWoman PDFDocument14 pages14 KnowledgeofContraceptivesMethodsandAppraisalofHealthEducationamongMarriedWoman PDFArdin MunrekPas encore d'évaluation
- Implicit Bias in Counseling For Permanent Contraception: Historical Context and Recommendations For CounselingDocument4 pagesImplicit Bias in Counseling For Permanent Contraception: Historical Context and Recommendations For CounselingyogurtPas encore d'évaluation
- Knowledge Attitudes and Practices Regarding ModernDocument7 pagesKnowledge Attitudes and Practices Regarding Modernnaasir abdiPas encore d'évaluation
- Published - POOJA UTTAM DABHADE - Post Natal Care Among Spouses (Europen Chemicle) (21!8!23)Document11 pagesPublished - POOJA UTTAM DABHADE - Post Natal Care Among Spouses (Europen Chemicle) (21!8!23)POOJA UTTAM DABHADEPas encore d'évaluation
- PDF MaternityCarePtEngagementStrategiesIHADocument29 pagesPDF MaternityCarePtEngagementStrategiesIHAv_ratPas encore d'évaluation
- Antenatal and Postnatal CareDocument12 pagesAntenatal and Postnatal CarehiwaPas encore d'évaluation
- Kanker ServiksDocument308 pagesKanker ServiksponekPas encore d'évaluation
- Checklist Dmpa EnglishDocument3 pagesChecklist Dmpa EnglishponekPas encore d'évaluation
- Sadiq KhanDocument5 pagesSadiq KhanponekPas encore d'évaluation
- Scientific Schedule: Alarm Course Day 1Document11 pagesScientific Schedule: Alarm Course Day 1ponekPas encore d'évaluation
- Preclinical Condition MagementDocument27 pagesPreclinical Condition MagementponekPas encore d'évaluation
- Analisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangDocument12 pagesAnalisis Pengendalian Alkes Farmasi Di Rs Pangkal PinangponekPas encore d'évaluation
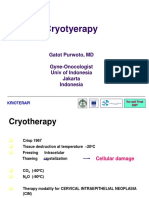
- CRYOTERAPI See&Treat GatotDocument20 pagesCRYOTERAPI See&Treat GatotponekPas encore d'évaluation
- Case-Digest-Imbong-V-Ochoa Part 2Document6 pagesCase-Digest-Imbong-V-Ochoa Part 2Kate Hazzle JandaPas encore d'évaluation
- Fix Makalah EnglishDocument25 pagesFix Makalah EnglishkezyaaaaaPas encore d'évaluation
- Global Health Issue: Kesehatan Ibu Dan AnakDocument67 pagesGlobal Health Issue: Kesehatan Ibu Dan AnakEra ZanaPas encore d'évaluation
- Significance of Health-Related Laws in Safeguarding People'S HealthDocument18 pagesSignificance of Health-Related Laws in Safeguarding People'S Healthjolina talledoPas encore d'évaluation
- GIM2002: Health, Disease and Lifestyle Chapter 1: Introduction HealthDocument20 pagesGIM2002: Health, Disease and Lifestyle Chapter 1: Introduction HealthFion TayPas encore d'évaluation
- SRH HERM Policy Brief A4Document4 pagesSRH HERM Policy Brief A4Sam TPas encore d'évaluation
- CHAPTER ONE - Doc..bakDocument27 pagesCHAPTER ONE - Doc..bakUsman Ahmad TijjaniPas encore d'évaluation
- Model United Nations MUN Study Guide For WHODocument21 pagesModel United Nations MUN Study Guide For WHOharit1248Pas encore d'évaluation
- Continuum of Care LancetDocument12 pagesContinuum of Care LancetNashria Rusdhy100% (1)
- ASHM Master Mentor Training PNGDocument4 pagesASHM Master Mentor Training PNGdaniel elakpaPas encore d'évaluation
- Say Hello To Our Body PDFDocument123 pagesSay Hello To Our Body PDFNatasha HadiwinataPas encore d'évaluation
- As RH PhilippinesDocument153 pagesAs RH PhilippinesAko Si XtianPas encore d'évaluation
- MCN Post Test IIDocument14 pagesMCN Post Test IIquidditch07Pas encore d'évaluation
- SRHR An Essential Element of UHC SupplementAndUniversalAccess 27-Online PDFDocument48 pagesSRHR An Essential Element of UHC SupplementAndUniversalAccess 27-Online PDFEmmanuelPas encore d'évaluation
- AEP - Teachers WorkbookDocument211 pagesAEP - Teachers Workbooksudharamalingam100% (1)
- A Two-Part Critique of The RH LawDocument13 pagesA Two-Part Critique of The RH LawCarlos Antonio P. Palad100% (1)
- NFDN 2006Document7 pagesNFDN 2006api-302133133100% (1)
- Special: Sexual HealthDocument1 pageSpecial: Sexual HealthbabyPas encore d'évaluation
- Nurlalili RahmiDocument10 pagesNurlalili RahmiEviza K. NadyaPas encore d'évaluation
- Final Manu Sex EdDocument29 pagesFinal Manu Sex Eddee jayPas encore d'évaluation
- Republic of The Philippines Province of Surigao Del Sur Municipality of HinatuanDocument13 pagesRepublic of The Philippines Province of Surigao Del Sur Municipality of HinatuanGLORIFE RIVERALPas encore d'évaluation
- Mulat Pinoy Year 3: Video Contest Content AnalysisDocument29 pagesMulat Pinoy Year 3: Video Contest Content AnalysisMulat Pinoy-Kabataan News NetworkPas encore d'évaluation
- The Health Benefits of Family Planning and Reproductive HealthDocument7 pagesThe Health Benefits of Family Planning and Reproductive HealtharmelgarPas encore d'évaluation
- Hina J. Talib (Eds.) - Adolescent Gynecology - A Clinical Casebook-Springer International Publishing (2018) PDFDocument281 pagesHina J. Talib (Eds.) - Adolescent Gynecology - A Clinical Casebook-Springer International Publishing (2018) PDFsalah subbahPas encore d'évaluation
- AYRH Final Print-Ready April 2011Document159 pagesAYRH Final Print-Ready April 2011Fentahun Ze WoinambaPas encore d'évaluation
- Reproductive Rights in NepalDocument30 pagesReproductive Rights in NepalRukmani KhadkaPas encore d'évaluation
- Skkri 2007Document225 pagesSkkri 2007sutopo patriajati100% (3)
- Public Health Laws in The PhilippinesDocument24 pagesPublic Health Laws in The PhilippinesKarylle PetilPas encore d'évaluation
- Illinois Insurance ComplaintDocument11 pagesIllinois Insurance ComplaintBasseemPas encore d'évaluation
- National Policy and Legislation in Relation To Maternal Health and WelfareDocument2 pagesNational Policy and Legislation in Relation To Maternal Health and WelfareKumar Suryavanshi89% (19)