Vous aimerez peut-être aussi
- 017 Muscle PhysiologyDocument62 pages017 Muscle Physiologyapi-23664998867% (3)
- Ms Cardiac and Smooth 325-327Document5 pagesMs Cardiac and Smooth 325-327api-236649988Pas encore d'évaluation
- Ms Contraction 300-307Document8 pagesMs Contraction 300-307api-236649988Pas encore d'évaluation
- Ms Reviewsummary 327-331Document5 pagesMs Reviewsummary 327-331api-236649988Pas encore d'évaluation
- Ms Performance 320-323Document5 pagesMs Performance 320-323api-236649988Pas encore d'évaluation
- 017 Review Ms ChaptmartinDocument13 pages017 Review Ms Chaptmartinapi-236649988Pas encore d'évaluation
- Heart Review Question1Document6 pagesHeart Review Question1api-236649988Pas encore d'évaluation
- 708-715 CardiodynamicsDocument8 pages708-715 Cardiodynamicsapi-236649988Pas encore d'évaluation
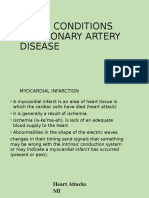
- 017 6 Hearrt ConditionsDocument11 pages017 6 Hearrt Conditionsapi-236649988Pas encore d'évaluation
- 017 5 Blood PressureDocument5 pages017 5 Blood Pressureapi-236649988Pas encore d'évaluation
- 697 702conductionDocument6 pages697 702conductionapi-236649988Pas encore d'évaluation
- 017 7 Heart Attack Coronary Artery Disease CadDocument7 pages017 7 Heart Attack Coronary Artery Disease Cadapi-236649988Pas encore d'évaluation
- 017 3 Conduction EkgDocument18 pages017 3 Conduction Ekgapi-236649988Pas encore d'évaluation
- 017 2 Coronary ArteriesDocument12 pages017 2 Coronary Arteriesapi-236649988Pas encore d'évaluation
- 017 Nails 017Document7 pages017 Nails 017api-236649988Pas encore d'évaluation
- 017 4 Heart SoundsDocument8 pages017 4 Heart Soundsapi-236649988Pas encore d'évaluation
- 017 1 Intro Heart AnatDocument33 pages017 1 Intro Heart Anatapi-236649988Pas encore d'évaluation
- 017 Infections and Allergies SkinDocument14 pages017 Infections and Allergies Skinapi-236649988Pas encore d'évaluation
- 017 Epidermis LayersDocument17 pages017 Epidermis Layersapi-236649988Pas encore d'évaluation
- Martin 017 HeartDocument58 pagesMartin 017 Heartapi-236649988Pas encore d'évaluation
- 017 BurnsDocument12 pages017 Burnsapi-236649988Pas encore d'évaluation
- Hair 017Document9 pagesHair 017api-236649988Pas encore d'évaluation
- Skin ColorDocument16 pagesSkin Colorapi-236649988Pas encore d'évaluation
- Integumentary System DisordersDocument15 pagesIntegumentary System Disordersapi-236649988Pas encore d'évaluation
- 017 Skin Intro FNDocument8 pages017 Skin Intro FNapi-236649988Pas encore d'évaluation
- Dermis HypodermisDocument9 pagesDermis Hypodermisapi-236649988Pas encore d'évaluation
- Glands 017Document11 pagesGlands 017api-236649988Pas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (399)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- Chapter 11. Cardiovascular-SystemDocument10 pagesChapter 11. Cardiovascular-SystemScianna Christel LastimosaPas encore d'évaluation
- Inner SmileDocument1 pageInner SmileIon ConstantinPas encore d'évaluation
- ECG Practise Exam Answers - 2019Document10 pagesECG Practise Exam Answers - 2019Ronak SinaeiPas encore d'évaluation
- 48 Hour Chick Reviewer PDFDocument5 pages48 Hour Chick Reviewer PDFSheanna May FuriaPas encore d'évaluation
- The Benefits of Chocolate in Daily LifeDocument3 pagesThe Benefits of Chocolate in Daily LifeAfiq SyahmiPas encore d'évaluation
- QP May-2013 Paper 2 PDFDocument20 pagesQP May-2013 Paper 2 PDFMoazzem HossainPas encore d'évaluation
- Dr. AsifDocument30 pagesDr. AsifUsman DastgirPas encore d'évaluation
- COmplications of HypertensionDocument32 pagesCOmplications of Hypertensionnananana123Pas encore d'évaluation
- 2010 JanDocument160 pages2010 JanalicePas encore d'évaluation
- Molecular Physiology of Cardiac Repolarization: Nerbonne, Jeanne M., and Robert S. KassDocument49 pagesMolecular Physiology of Cardiac Repolarization: Nerbonne, Jeanne M., and Robert S. Kassrizki sundusiasihPas encore d'évaluation
- Physical Education UGC NET Examination Question Paper 2 2006 June PDFDocument24 pagesPhysical Education UGC NET Examination Question Paper 2 2006 June PDFsandwwpPas encore d'évaluation
- Questions - Homework - 10th - Science - 2021-11-24T05 - 44Document12 pagesQuestions - Homework - 10th - Science - 2021-11-24T05 - 44Saurabh BhattacharyaPas encore d'évaluation
- Yyyyy Y YDocument49 pagesYyyyy Y YSiva Nantham100% (1)
- Anatomy and Physiology of Farm AnimalsDocument169 pagesAnatomy and Physiology of Farm AnimalsKRIZZAPEARL VER100% (1)
- Application of King's Theory of Goal Attainment in Miocard Infarct PatientDocument34 pagesApplication of King's Theory of Goal Attainment in Miocard Infarct PatientYulis HatiPas encore d'évaluation
- Intra Aortic Balloon Pump (IABP) 2009Document57 pagesIntra Aortic Balloon Pump (IABP) 2009nurminsyahPas encore d'évaluation
- Ecocardiografia FetalDocument385 pagesEcocardiografia Fetalyelsinosmin romeroalvaradoPas encore d'évaluation
- Shock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentDocument64 pagesShock - Types Pathophysiology and Management: DR - Ravichandra Kumar Anaesthesia ResidentHarika BandaruPas encore d'évaluation
- Updated - Prioritization of ProblemsDocument1 pageUpdated - Prioritization of ProblemsKaycelyn JimenezPas encore d'évaluation
- Anesthesia Considerations During Cytoreductive SurDocument9 pagesAnesthesia Considerations During Cytoreductive Surdrardigustian2986Pas encore d'évaluation
- Cardiac Arrhythmia Detection Using Deep LearningDocument9 pagesCardiac Arrhythmia Detection Using Deep LearningRevati WablePas encore d'évaluation
- IM Shelf - AmbossDocument61 pagesIM Shelf - AmbossHaadi AliPas encore d'évaluation
- EstateDocument38 pagesEstateMichael_Lee_RobertsPas encore d'évaluation
- Key Advances in Medicine 2015Document98 pagesKey Advances in Medicine 2015Alain Riveros100% (2)
- MJPJAY Procedures 996Document58 pagesMJPJAY Procedures 996bhushan adhariPas encore d'évaluation
- Marieb ch11bDocument28 pagesMarieb ch11bapi-229554503Pas encore d'évaluation
- Mitral Valve StenosisDocument2 pagesMitral Valve StenosisSrhi NurhayatiiPas encore d'évaluation
- 2015 Akutni Koronarni SindromDocument98 pages2015 Akutni Koronarni SindromIvanMihailovicPas encore d'évaluation
- NCM 118 Skills Lab (Week 8)Document4 pagesNCM 118 Skills Lab (Week 8)kPas encore d'évaluation
- Lab 2Document6 pagesLab 2api-272723910Pas encore d'évaluation