Vous aimerez peut-être aussi
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Admission Nurses Notes SampleDocument3 pagesAdmission Nurses Notes SampleAaron Wallace88% (8)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Phelebotomy Answers 01 2018Document61 pagesPhelebotomy Answers 01 2018Aaron Wallace100% (1)
- Intro To EugenicsDocument16 pagesIntro To EugenicsJesus LivesPas encore d'évaluation
- DLM JOY Bread Maker Recipe BookDocument35 pagesDLM JOY Bread Maker Recipe BookmimaPas encore d'évaluation
- Risk Assessment Questions and Answers 1624351390Document278 pagesRisk Assessment Questions and Answers 1624351390Firman Setiawan100% (1)
- Vascular Disorder Case StudyDocument3 pagesVascular Disorder Case StudyAaron Wallace100% (1)
- Dental Juris and Practice MGT Board 2008Document14 pagesDental Juris and Practice MGT Board 2008Anonymous FwwfR650% (2)
- HERING Law FalseDocument5 pagesHERING Law FalseVirag PatilPas encore d'évaluation
- Homeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1Document6 pagesHomeopathic Remedy Pictures Alexander Gothe Julia Drinnenberg.04000 1BhargavaPas encore d'évaluation
- Lüscher Colour TestDocument1 pageLüscher Colour TestVicente Sebastián Márquez LecarosPas encore d'évaluation
- Office: The of The SecretaryDocument20 pagesOffice: The of The SecretaryJustine KimPas encore d'évaluation
- Hazops Should Be Fun - The Stream-Based HazopDocument77 pagesHazops Should Be Fun - The Stream-Based HazopHector Tejeda100% (1)
- Renr Practice Test 11Document17 pagesRenr Practice Test 11Aaron Wallace92% (12)
- Renr Review Program 2016Document8 pagesRenr Review Program 2016Aaron Wallace100% (2)
- Mobile Health Clinic InitiativeDocument47 pagesMobile Health Clinic InitiativededdyPas encore d'évaluation
- April CXC Exam Plus Answers 2016 (30753)Document15 pagesApril CXC Exam Plus Answers 2016 (30753)Aaron Wallace90% (10)
- Nursing Council CXC Past Paper MCQ (1) (319) IMPORTANTDocument25 pagesNursing Council CXC Past Paper MCQ (1) (319) IMPORTANTAaron Wallace88% (32)
- Apirl 2001 Paper 2 (CL)Document15 pagesApirl 2001 Paper 2 (CL)Aaron Wallace100% (1)
- Nurs Council TopicsDocument1 pageNurs Council TopicsAaron Wallace100% (1)
- What Is AdpieDocument5 pagesWhat Is AdpieAaron WallacePas encore d'évaluation
- Psychology TheoriesDocument7 pagesPsychology TheoriesAaron WallacePas encore d'évaluation
- Cardiac System MedicationsDocument4 pagesCardiac System MedicationsfranjoyPas encore d'évaluation
- Asthma MedicationsDocument3 pagesAsthma MedicationsAaron WallacePas encore d'évaluation
- A Kestrel For A Knave - WikipediaDocument26 pagesA Kestrel For A Knave - WikipediaAaron WallacePas encore d'évaluation
- 1503 KJSDLJFLSDF X10Document219 pages1503 KJSDLJFLSDF X10Aaron WallacePas encore d'évaluation
- Angina ManagementDocument14 pagesAngina ManagementAaron WallacePas encore d'évaluation
- Scan0010 RotatedDocument12 pagesScan0010 RotatedAaron Wallace100% (3)
- International Women Day 2017Document1 pageInternational Women Day 2017Aaron WallacePas encore d'évaluation
- Hint For AdmissionDocument5 pagesHint For AdmissionAaron WallacePas encore d'évaluation
- Dry Swabs: Diascan StripsDocument5 pagesDry Swabs: Diascan StripsAaron WallacePas encore d'évaluation
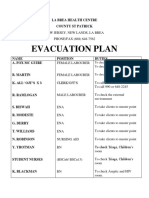
- Evacuation Plan: La Brea Health Centre County ST PatrickDocument2 pagesEvacuation Plan: La Brea Health Centre County ST PatrickAaron WallacePas encore d'évaluation
- Labels For WardsDocument8 pagesLabels For WardsAaron WallacePas encore d'évaluation
- October 2000 Paper 4Document14 pagesOctober 2000 Paper 4Aaron Wallace100% (1)
- Asthma MedicationsDocument3 pagesAsthma MedicationsAaron WallacePas encore d'évaluation
- April 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Document10 pagesApril 1999 Paper 1 Clinical Nursing Essay - Type Test Items: Scenario 1 Item 1Aaron WallacePas encore d'évaluation
- Key April 2001 Paper 3Document8 pagesKey April 2001 Paper 3Aaron WallacePas encore d'évaluation
- EdCaN Specialty Module 4Document23 pagesEdCaN Specialty Module 4cindy8127Pas encore d'évaluation
- Chemical Biology: Semester - Iii and Vii 2017-18Document12 pagesChemical Biology: Semester - Iii and Vii 2017-18Yogesh ShekhawatPas encore d'évaluation
- 9401-Article Text-17650-1-10-20200718Document5 pages9401-Article Text-17650-1-10-20200718agail balanagPas encore d'évaluation
- Antitrombotik, PPT 7Document66 pagesAntitrombotik, PPT 7Rizky Saraswati IndraputriPas encore d'évaluation
- Pulpal DiseasesDocument34 pagesPulpal Diseasessamar yousif mohamedPas encore d'évaluation
- Two Dimensional and M-Mode Echocardiography - BoonDocument112 pagesTwo Dimensional and M-Mode Echocardiography - BoonRobles RobertoPas encore d'évaluation
- The Health Promotion Model (Nola J. Pender) : SupratmanDocument11 pagesThe Health Promotion Model (Nola J. Pender) : SupratmanNugraha PratamaPas encore d'évaluation
- BB - Self AuditDocument18 pagesBB - Self AuditFe Rackle Pisco JamerPas encore d'évaluation
- Botswana Ref Ranges PaperDocument7 pagesBotswana Ref Ranges PaperMunyaradzi MangwendezaPas encore d'évaluation
- Building and Handling Therapeutic Closeness in The Therapist-ClientDocument9 pagesBuilding and Handling Therapeutic Closeness in The Therapist-ClientRaphaele ColferaiPas encore d'évaluation
- Talent MappingDocument18 pagesTalent MappingSoumya RanjanPas encore d'évaluation
- Biocontrol in Disease SugarcaneDocument11 pagesBiocontrol in Disease SugarcaneAlbar ConejoPas encore d'évaluation
- Jurnal BM 7Document18 pagesJurnal BM 7Nitya WirasasiPas encore d'évaluation
- Matter For PGDIPC Course PromotionDocument1 pageMatter For PGDIPC Course PromotionAnkur VasudevaPas encore d'évaluation
- Research ProposalDocument3 pagesResearch Proposalapi-446880170Pas encore d'évaluation
- A Guide For The Assessment and Management of Post-Obstructive DiuresisDocument3 pagesA Guide For The Assessment and Management of Post-Obstructive DiuresisRara Aulia IIPas encore d'évaluation
- Food Data Chart - ZincDocument6 pagesFood Data Chart - Zinctravi95Pas encore d'évaluation
- Kraniotomi DekompresiDocument17 pagesKraniotomi DekompresianamselPas encore d'évaluation
- PIIS0261561422000668 Micronitrientes: RequerimientosDocument70 pagesPIIS0261561422000668 Micronitrientes: Requerimientossulemi castañonPas encore d'évaluation
- Gefico Maritime SectorDocument28 pagesGefico Maritime SectorAugustine Dharmaraj100% (1)