Vous aimerez peut-être aussi
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceD'EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceÉvaluation : 4 sur 5 étoiles4/5 (895)
- Doctor Statement Ssa 787Document3 pagesDoctor Statement Ssa 787Richard GuthPas encore d'évaluation
- Never Split the Difference: Negotiating As If Your Life Depended On ItD'EverandNever Split the Difference: Negotiating As If Your Life Depended On ItÉvaluation : 4.5 sur 5 étoiles4.5/5 (838)
- Tim Richardson TMA02Document6 pagesTim Richardson TMA02Tim RichardsonPas encore d'évaluation
- The Yellow House: A Memoir (2019 National Book Award Winner)D'EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Évaluation : 4 sur 5 étoiles4/5 (98)
- DiseaseDocument3 pagesDiseaseTyron KristianPas encore d'évaluation
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeD'EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeÉvaluation : 4 sur 5 étoiles4/5 (5794)
- PromixineDocument2 pagesPromixineStelaA1Pas encore d'évaluation
- Shoe Dog: A Memoir by the Creator of NikeD'EverandShoe Dog: A Memoir by the Creator of NikeÉvaluation : 4.5 sur 5 étoiles4.5/5 (537)
- PDSA Examples: PlanDocument6 pagesPDSA Examples: PlanTrà My Lê MỹPas encore d'évaluation
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaD'EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaÉvaluation : 4.5 sur 5 étoiles4.5/5 (266)
- GSRC Trans Resource Guide (2015-2016)Document19 pagesGSRC Trans Resource Guide (2015-2016)Merissa Taylor-Meissner100% (1)
- The Little Book of Hygge: Danish Secrets to Happy LivingD'EverandThe Little Book of Hygge: Danish Secrets to Happy LivingÉvaluation : 3.5 sur 5 étoiles3.5/5 (400)
- Jaw LashDocument16 pagesJaw LashSven BivalPas encore d'évaluation
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureD'EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureÉvaluation : 4.5 sur 5 étoiles4.5/5 (474)
- Oxygen-Induced Hypercapnia in COPD PDFDocument4 pagesOxygen-Induced Hypercapnia in COPD PDFsatyagraha84Pas encore d'évaluation
- Ret Dem Bed Bath Hair Shampoo WUPDocument4 pagesRet Dem Bed Bath Hair Shampoo WUPCarissa De Luzuriaga-BalariaPas encore d'évaluation
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryD'EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryÉvaluation : 3.5 sur 5 étoiles3.5/5 (231)
- Interview QuestionsDocument5 pagesInterview QuestionsFlorin NovacPas encore d'évaluation
- Grit: The Power of Passion and PerseveranceD'EverandGrit: The Power of Passion and PerseveranceÉvaluation : 4 sur 5 étoiles4/5 (588)
- What Are Moral DilemmasDocument7 pagesWhat Are Moral DilemmasMary Anne Rocafor NaelgasPas encore d'évaluation
- The Emperor of All Maladies: A Biography of CancerD'EverandThe Emperor of All Maladies: A Biography of CancerÉvaluation : 4.5 sur 5 étoiles4.5/5 (271)
- Care Map UtiDocument1 pageCare Map UtiJonathonPas encore d'évaluation
- The Unwinding: An Inner History of the New AmericaD'EverandThe Unwinding: An Inner History of the New AmericaÉvaluation : 4 sur 5 étoiles4/5 (45)
- Revised Instrument Packet 2Document44 pagesRevised Instrument Packet 2Abdiaziz Walhad0% (1)
- On Fire: The (Burning) Case for a Green New DealD'EverandOn Fire: The (Burning) Case for a Green New DealÉvaluation : 4 sur 5 étoiles4/5 (74)
- KyphosisDocument4 pagesKyphosisclubsanatatePas encore d'évaluation
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersD'EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersÉvaluation : 4.5 sur 5 étoiles4.5/5 (345)
- Oregon V Azar ComplaintDocument109 pagesOregon V Azar ComplaintHonolulu Star-Advertiser100% (1)
- Team of Rivals: The Political Genius of Abraham LincolnD'EverandTeam of Rivals: The Political Genius of Abraham LincolnÉvaluation : 4.5 sur 5 étoiles4.5/5 (234)
- Nurse's Role in Medication ReconciliationDocument24 pagesNurse's Role in Medication ReconciliationDeamon SakaragaPas encore d'évaluation
- Republic Act No 9288Document4 pagesRepublic Act No 9288Janela BaisPas encore d'évaluation
- The Neurobiology of We - Patty de LlosaDocument4 pagesThe Neurobiology of We - Patty de LlosaFernando Morari100% (3)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreD'EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreÉvaluation : 4 sur 5 étoiles4/5 (1090)
- Procedure Error RCTDocument4 pagesProcedure Error RCTRolzilah RohaniPas encore d'évaluation
- Adoption and Spread of Innovation in The NHS: This Content Relates To The Following TopicsDocument4 pagesAdoption and Spread of Innovation in The NHS: This Content Relates To The Following Topicszeze_13Pas encore d'évaluation
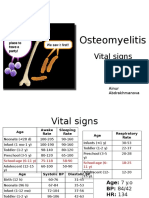
- PBL 2 - OsteomyelitisDocument10 pagesPBL 2 - OsteomyelitisAinur AbdrakhmanovaPas encore d'évaluation
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyD'EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyÉvaluation : 3.5 sur 5 étoiles3.5/5 (2259)
- Literature Review Diabetes DistressDocument7 pagesLiterature Review Diabetes DistressDebby Syahru RomadlonPas encore d'évaluation
- First Aid Vocabulary Part 1Document2 pagesFirst Aid Vocabulary Part 1Marina WindsorPas encore d'évaluation
- Haggard & Chambon 2012 Sense of AgencyDocument3 pagesHaggard & Chambon 2012 Sense of AgencyhooriePas encore d'évaluation
- Effectiveness of Neural Mobilization in The ManageDocument2 pagesEffectiveness of Neural Mobilization in The ManagechristinePas encore d'évaluation
- Hematology - Oncology GlossaryDocument18 pagesHematology - Oncology GlossaryFran CescaPas encore d'évaluation
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)D'EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Évaluation : 4.5 sur 5 étoiles4.5/5 (121)
- HCL Healthcare SIP ReportDocument65 pagesHCL Healthcare SIP ReportPuneet GoyalPas encore d'évaluation
- Interproximal Tissue Dimensions in Relation To Adjacent Implants in The Anterior Maxilla - Clinical Observations and Patient Aesthetic EvaluationDocument11 pagesInterproximal Tissue Dimensions in Relation To Adjacent Implants in The Anterior Maxilla - Clinical Observations and Patient Aesthetic EvaluationEduardo AyubPas encore d'évaluation
- Ulnar Nerve Injury, Diagnosis and TreatmentDocument30 pagesUlnar Nerve Injury, Diagnosis and TreatmentsherysheryyPas encore d'évaluation
- Her Body and Other Parties: StoriesD'EverandHer Body and Other Parties: StoriesÉvaluation : 4 sur 5 étoiles4/5 (821)